Trojani Alessandra, Beghini Alessandro, Bossi Luca Emanuele, Stefanucci Marta Rachele, Palumbo Cassandra, Greco Antonino, Frustaci Annamaria, Di Camillo Barbara, Cairoli Roberto
Niguarda Hospital, Department of Hematology and Oncology, Milano, Italy.
Department of Health Sciences, University of Milano, Milano, Italy.
Cancer Med. 2024 Dec;13(24):e70525. doi: 10.1002/cam4.70525.
Despite recurrent and activating mutations, including MYD88, CXCR4, ARID1A, KMT2D, and CD79B were identified, the genetic basis for Waldenström's Macroglobulinemia (WM) and the risk of progression of IgM MGUS to WM remain to be fully elucidated.
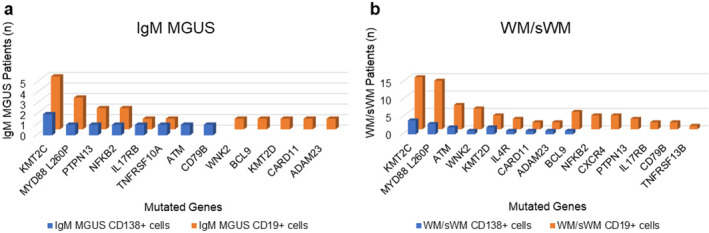
We investigated the mutation status of WM (n = 8), sWM (n = 7), and IgM MGUS (n = 5) patients, by performing high-throughput targeted AmpliSeq NGS on 117 target genes. Specifically, we analyzed the CD19+ cells from 15 WM/sWM patients and five IgM MGUS patients. We also analyzed the CD138+ cells from four WM/sWM patients and two IgM MGUS patients.
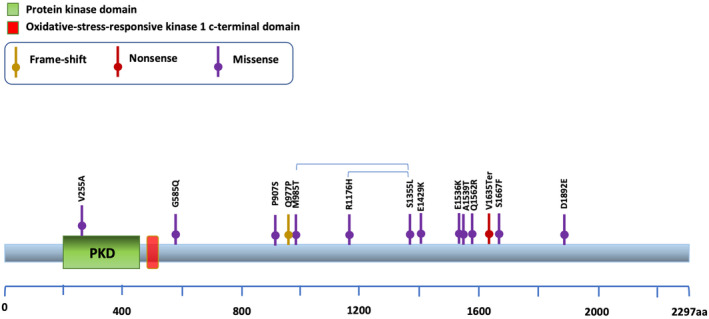
We detected the classic mutation MYD88L265P in 93% of WM/sWM and in 60% of IgM MGUS patients. The CXCR4S338Ter mutation was identified in 26% of WM/sWM patients, whereas it was undetectable in IgM MGUS subjects. Interestingly, we identified new mutated genes, including WNK2 somatic mutations affecting 46% of WM/sWM patients, for which a recurrent allelic variant (V1635Ter) was observed in this cohort. Moreover, sequencing evaluation revealed recurrently frameshift or missense mutations involving NFKB2 (L473Afs) in 60% of IgM MGUS and 20% of WM/sWM, PTPN13 (P1546Tfs) in 20% of IgM MGUS and 7% of WM/sWM, CARD11 (S622del) in 20% of IgM MGUS and 20% of WM/sWM, KMT2C (I823T) in all IgM MGUS and 93% of WM/sWM, and ATM in 20% of IgM MGUS and 47% of WM/sWM patients.
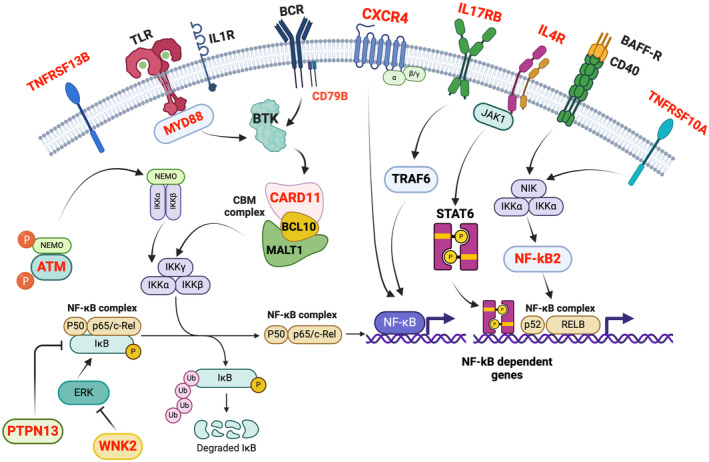
In conclusion, we uncovered new insights into the mutational landscape of WM, depicting a more complex involvement of the NF-kB pathway, and providing evidence of the recurrence of some variants (MYD88, IL17RB, NFKB2, ATM, CARD11, PTPN13, and WNK2) also in IgM MGUS.
尽管已鉴定出包括MYD88、CXCR4、ARID1A、KMT2D和CD79B在内的复发性和激活突变,但华氏巨球蛋白血症(WM)的遗传基础以及IgM意义未明的单克隆丙种球蛋白病(IgM MGUS)进展为WM的风险仍有待充分阐明。
我们通过对117个靶基因进行高通量靶向扩增子测序(AmpliSeq NGS),研究了WM患者(n = 8)、冒烟型WM(sWM)患者(n = 7)和IgM MGUS患者(n = 5)的突变状态。具体而言,我们分析了15例WM/sWM患者和5例IgM MGUS患者的CD19+细胞。我们还分析了4例WM/sWM患者和2例IgM MGUS患者的CD138+细胞。
我们在93%的WM/sWM患者和60%的IgM MGUS患者中检测到经典突变MYD88L265P。在26%的WM/sWM患者中鉴定出CXCR4S338Ter突变,而在IgM MGUS患者中未检测到。有趣的是,我们鉴定出了新的突变基因,包括影响46%的WM/sWM患者的WNK2体细胞突变,在该队列中观察到了一个复发性等位基因变异(V1635Ter)。此外测序评估显示,60%的IgM MGUS患者和20%的WM/sWM患者存在涉及NFKB2(L473Afs)的复发性移码或错义突变,20%的IgM MGUS患者和7%的WM/sWM患者存在PTPN13(P1546Tfs)突变,20%的IgM MGUS患者和20%的WM/sWM患者存在CARD11(S622del)突变,所有IgM MGUS患者和93%的WM/sWM患者存在KMT2C(I823T)突变,20%的IgM MGUS患者和47%的WM/sWM患者存在ATM突变。
总之,我们揭示了WM突变格局的新见解,描绘了NF-κB通路更复杂的参与情况,并提供了一些变异(MYD家族88、IL17RB、NFKB2、ATM、CARD11、PTPN13和WNK2)在IgM MGUS中也存在复发的证据。