Brar Shanjot, Kang Mehima, Sodhi Amit, Deyell Marc W, Laksman Zachary, Andrade Jason G, Bennett Matthew T, Krahn Andrew D, Yeung-Lai-Wah John, Bennett Richard G, Barlow Amanda, Grewal Jasmine, Sathananthan Gnalini, Chakrabarti Santabhanu
Department of Medicine, University of British Columbia, Vancouver, Canada.
Division of Cardiology, Department of Medicine, University of British Columbia, Vancouver, Canada.
Int J Cardiol Congenit Heart Dis. 2024 Mar 26;16:100508. doi: 10.1016/j.ijcchd.2024.100508. eCollection 2024 Jun.
Surgically repaired Tetralogy of Fallot (rTOF) is associated with progressive right ventricular hypertrophy (RVH) and dilation (RVD). Accurate estimation of RVH/RVD is vital for the ongoing management of this patient population. The utility of the ECG in evaluating patients with rTOF with pre-existing right bundle branch block (RBBB) has not been studied. We aimed to determine the sensitivity/specificity of currently established ECG criteria in detecting RVH/RVD in this patient population.
We included consecutive patients diagnosed with rTOF who underwent CMR performed at our regional referral centre between January 2012 and December 2019. Each CMR was assessed for LVH, LVD, RVH and or RVD. The ECG corresponding to the CMR was then used to determine RVH/LVH for specificity and sensitivity analysis.
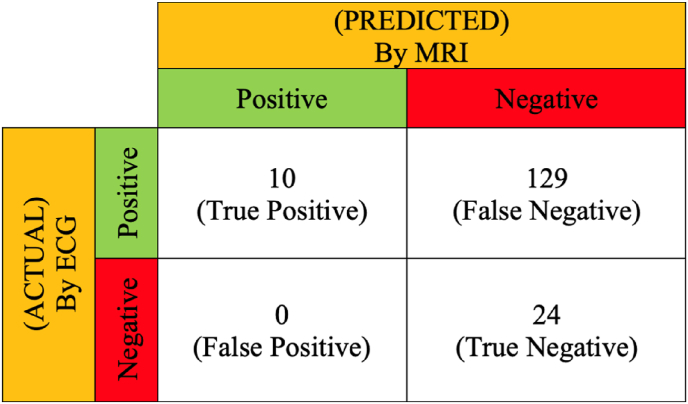
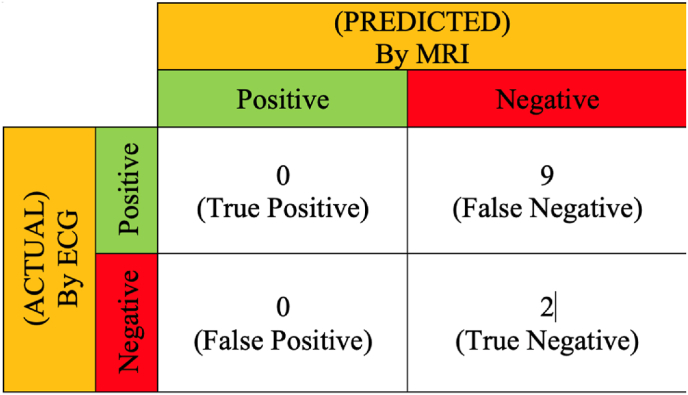
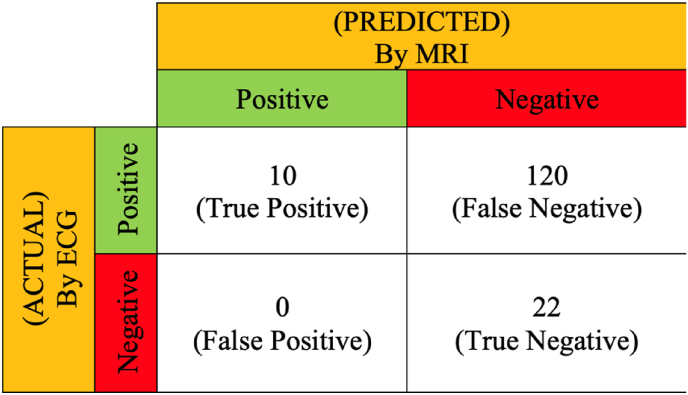
Our study included 163 consecutive rTOF patients. The specificity for ECG-based criteria for LVH was 100.00% (95% C.I. (87.75, 100.00)), and the sensitivity was 7.19% (95% C.I. (3.15, 12.83)). When RBBB was present, specificity for RVH was 100.00% (95% C.I. (84.56, 100.00)), and sensitivity was 7.69% (95% C.I. (3.75, 13.69)). When RBBB was absent, specificity for RVH was 100.00% (95% C.I. (15.81, 100.00)), and sensitivity was 0.00% (95% C.I. (0.00, 33.63)). A regression model with the entire group of 163 ToF patients, based on the Sokolow-Lyon criterion (sum of R in V1 + S in V5/V6), produced a new suggested criterion for the diagnosis of RVH in patients with rTOF, which was a sum of R in V1 + S in V5/V6 greater than 13.25 mm. This model's sensitivity for RVH detection was 69.1%, and specificity was 36.8%.
Standard ECG voltage criteria have poor sensitivity for detecting right and left ventricular chamber hypertrophy and dilatation in patients with rTOF, so current ECG criteria should not be used to monitor RVH/RVD in this patient population.
法洛四联症外科修复术后(rTOF)与进行性右心室肥厚(RVH)和扩张(RVD)相关。准确评估RVH/RVD对于该患者群体的持续管理至关重要。心电图在评估合并预先存在右束支传导阻滞(RBBB)的rTOF患者中的作用尚未得到研究。我们旨在确定当前既定心电图标准在检测该患者群体的RVH/RVD中的敏感性/特异性。
我们纳入了2012年1月至2019年12月期间在我们地区转诊中心接受心脏磁共振成像(CMR)检查的连续诊断为rTOF的患者。对每次CMR评估左心室肥厚(LVH)、左心室扩张(LVD)、RVH和/或RVD。然后使用与CMR对应的心电图来确定RVH/LVH以进行特异性和敏感性分析。
我们的研究包括163例连续的rTOF患者。基于心电图的LVH标准的特异性为100.00%(95%置信区间(87.75, 100.00)),敏感性为7.19%(95%置信区间(3.15, 12.83))。当存在RBBB时,RVH的特异性为100.00%(95%置信区间(84.56, 100.00)),敏感性为7.69%(95%置信区间(3.75, 13.69))。当不存在RBBB时,RVH的特异性为100.00%(95%置信区间(15.81, 100.00)),敏感性为0.00%(95%置信区间(0.00, 33.63))。基于Sokolow-Lyon标准(V1导联R波 + V5/V6导联S波之和),对163例法洛四联症患者的整个队列建立回归模型,得出了一个新的用于诊断rTOF患者RVH的建议标准,即V1导联R波 + V5/V6导联S波之和大于13.25毫米。该模型检测RVH的敏感性为69.1%,特异性为36.8%。
标准心电图电压标准在检测rTOF患者的右心室和左心室肥厚及扩张方面敏感性较差,因此当前心电图标准不应用于监测该患者群体的RVH/RVD。