Last Anna R, Shafi Abdurahman Oumer, Greenland Katie, Robinson Ailie, Collin Claire, Czerniewska Alexandra, Etu Edao Sinba, Versteeg Bart, Butcher Robert, Guye Meseret, Legesse Demitu, Nuri Kedir Temam, Shuka Gemeda, Haji Mohammed Yousuf Munira, Dheressa Gaddisa, Dumessa Gebeyehu, Akalu Melesse, Tadesse Mesfin, Adugna Kumsa Dereje, Seife Gebretsadik Fikre, Abashawl Aida, Habtamu Esmael, Sarah Virginia, Alemayehu Wondu, Solomon Anthony, Weiss Helen Anne, Logan James G, Macleod David, Burton Matthew J
Clinical Research Department, London School of Hygiene & Tropical Medicine, London, UK
Clinical Research Department, London School of Hygiene & Tropical Medicine, London, UK.
BMJ Open. 2024 Dec 23;14(12):e084478. doi: 10.1136/bmjopen-2024-084478.
Trachoma is caused by the bacterium (). The WHO recommends the SAFE strategy for trachoma elimination: Surgery for trichiasis, Antibiotics, Facial cleanliness and Environmental improvement. Multiple rounds of SAFE implementation have proven insufficient to eliminate trachoma in Ethiopia, where over 50% of the global trachoma burden remains. More effective antibiotic treatment schedules and transmission-suppressing approaches are needed. The aim of stronger SAFE is to evaluate the impact of a novel package of interventions to strengthen the A, F and E of SAFE on the prevalence of ocular and trachoma in Oromia, Ethiopia.
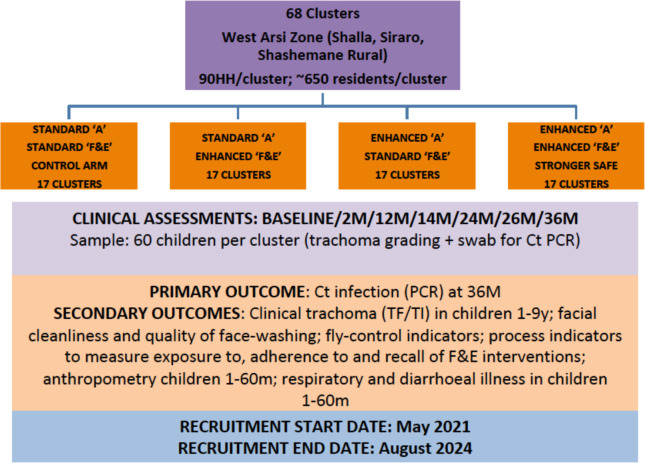
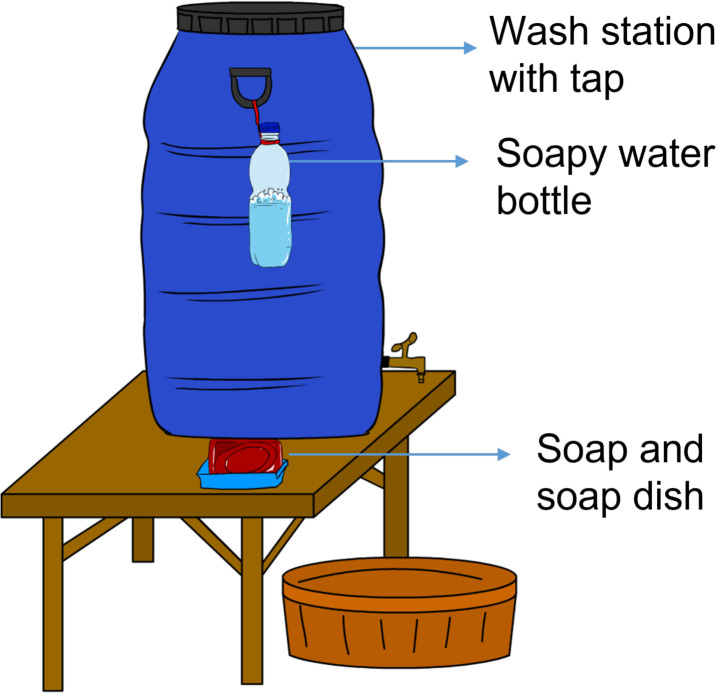
68 clusters were randomised in a 1:1:1:1 ratio to one of (1) standard A/standard F&E (standard SAFE), (2) standard A/enhanced F&E, (3) enhanced A/standard F&E or (4) enhanced A/enhanced F&E (stronger SAFE). Enhanced A includes two height-based doses of oral azithromycin (equivalent to 20 mg/kg) given as single doses 2 weeks apart, as mass drug administration, annually. Enhanced F&E includes fly control measures (permethrin-treated headwear and odour-baited traps) and face-washing hygiene behaviour change implemented at household level in selected communities. The interventions will be implemented and reinforced over 3 years.The primary outcome is the prevalence of ocular by quantitative PCR in children aged 1-9 years at 36 months. A key secondary outcome is the prevalence of active (inflammatory) trachoma in the same children, assessed by validated trachoma graders and conjunctival photography. Laboratory technicians and photo-graders are masked to treatment allocation. Other important secondary analyses include process evaluations, assessment of behaviour change, fly indicators, adherence and coverage of interventions and a cost analysis.
Study protocols have been approved by the National Research Ethics Review Committee of the Ethiopian Ministry of Science and Higher Education and the London School of Hygiene & Tropical Medicine Ethics Committee. An independent data safety and monitoring board oversees the trial. Results will be disseminated through peer-reviewed publications, presentations and reports.
ISRCTN40760473.
沙眼由 () 细菌引起。世界卫生组织推荐采用SAFE策略消除沙眼:倒睫手术、抗生素治疗、面部清洁和环境改善。事实证明,在埃塞俄比亚,多轮实施SAFE策略不足以消除沙眼,该国仍负担着全球超过50%的沙眼病例。因此需要更有效的抗生素治疗方案和抑制传播的方法。强化SAFE策略的目的是评估一套新的干预措施对加强SAFE策略中的A、F和E要素的影响,这些措施针对埃塞俄比亚奥罗米亚州的儿童沙眼患病率和沙眼情况。
68个群组按1:1:1:1的比例随机分为以下四组之一:(1)标准A/标准F&E(标准SAFE),(2)标准A/强化F&E,(3)强化A/标准F&E,或(4)强化A/强化F&E(强化SAFE)。强化A包括每年进行一次群体药物管理,以间隔2周的单剂量形式给予两剂基于身高的口服阿奇霉素(相当于20mg/kg)。强化F&E包括在选定社区的家庭层面实施的苍蝇控制措施(经氯菊酯处理的头饰和诱蝇器)以及洗脸卫生行为改变。这些干预措施将在3年内实施并强化。主要结局是36个月时1至9岁儿童通过定量PCR检测的沙眼衣原体患病率。一个关键的次要结局是通过经验证的沙眼分级人员和结膜摄影评估的同一批儿童中活动性(炎性)沙眼的患病率。实验室技术人员和照片分级人员对治疗分配情况不知情。其他重要的次要分析包括过程评估、行为改变评估、苍蝇指标、干预措施的依从性和覆盖率以及成本分析。
研究方案已获得埃塞俄比亚科学与高等教育部国家研究伦理审查委员会以及伦敦卫生与热带医学院伦理委员会的批准。一个独立的数据安全和监测委员会监督该试验。研究结果将通过同行评审的出版物、报告和演讲进行传播。
ISRCTN407604