Beitollahi Ariya, Berry Hunter, Gulotta Paul, Morales Robert, Milburn James
The University of Queensland Medical School, Ochsner Clinical School, New Orleans, LA.
Department of Radiology, Ochsner Clinic Foundation, New Orleans, LA.
Ochsner J. 2024 Winter;24(4):298-302. doi: 10.31486/toj.24.0027.
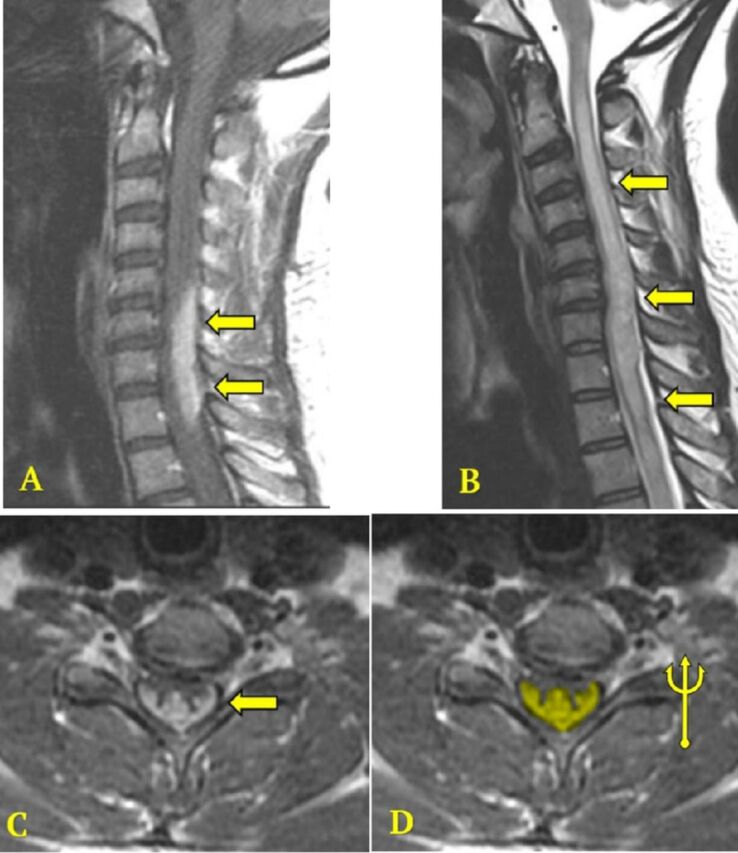
Spinal cord sarcoidosis, an uncommon manifestation of neurosarcoidosis, presents diagnostic and therapeutic challenges because the condition is rare and has diverse clinical manifestations that can mimic other conditions such as multiple sclerosis and neuromyelitis optica spectrum disorder. A middle-aged African American female with a history of idiopathic intracranial hypertension and hydrocephalus with ventriculoperitoneal shunt presented with progressive, predominantly left-sided gait instability, weakness, and paresthesia. Cerebrospinal fluid showed lymphocytosis, red blood cells, elevated oligoclonal bands, and elevated kappa free light chains, concerning for multiple sclerosis. Neuromyelitis optica spectrum disorder testing was negative. Magnetic resonance imaging (MRI) demyelination protocol revealed normal brain imaging and a longitudinally extensive spinal cord lesion with the distinctive trident sign on contrast-enhanced axial views, consistent with spinal cord sarcoidosis. The patient was treated with intravenous methylprednisolone for 5 days, resulting in improved lower extremity strength, but ataxia and sensory deficits, especially proprioception, persisted. Follow-up imaging and examinations demonstrated continued spinal cord involvement with minimal improvement despite treatment. Current management guidelines for spinal cord sarcoidosis are based on limited evidence, necessitating further research to establish optimal protocols. The trident sign on MRI may distinguish spinal cord sarcoidosis from conditions such as multiple sclerosis and neuromyelitis optica spectrum disorder. Early radiologic detection could improve outcomes and reduce long-term neurologic deficits. A comprehensive multidisciplinary approach is essential for effective, patient-centered care planning.
脊髓结节病是神经结节病的一种罕见表现形式,因其罕见且具有多种可模仿其他病症(如多发性硬化症和视神经脊髓炎谱系障碍)的临床表现,故而在诊断和治疗方面面临挑战。一名患有特发性颅内高压和脑积水并接受脑室腹腔分流术的中年非裔美国女性,出现了进行性的、主要为左侧的步态不稳、虚弱和感觉异常。脑脊液显示淋巴细胞增多、红细胞、寡克隆带升高以及κ游离轻链升高,这让人担心是多发性硬化症。视神经脊髓炎谱系障碍检测呈阴性。磁共振成像(MRI)脱髓鞘检查显示脑部成像正常,脊髓有一个纵向广泛的病变,在增强轴向视图上有独特的三叉戟征,符合脊髓结节病。该患者接受了5天的静脉注射甲泼尼龙治疗,下肢力量有所改善,但共济失调和感觉缺陷,尤其是本体感觉,仍然存在。随访成像和检查显示尽管进行了治疗,但脊髓仍持续受累,改善甚微。目前脊髓结节病的管理指南基于有限的证据,需要进一步研究以制定最佳方案。MRI上的三叉戟征可能有助于将脊髓结节病与多发性硬化症和视神经脊髓炎谱系障碍等病症区分开来。早期的影像学检测可以改善预后并减少长期神经功能缺损。全面的多学科方法对于以患者为中心的有效护理规划至关重要。