Zhao Junjie, Sun Yong, Tang Jing, Guo Kai, Zhuge Jiancheng, Fang Honglong
Zhejiang Chinese Medical University, Hangzhou, 310053, Zhejiang, China.
Quzhou Hospital of Traditional Chinese Medicine, Quzhou, 324000, Zhejiang, China.
Sci Rep. 2024 Dec 30;14(1):31808. doi: 10.1038/s41598-024-83038-7.
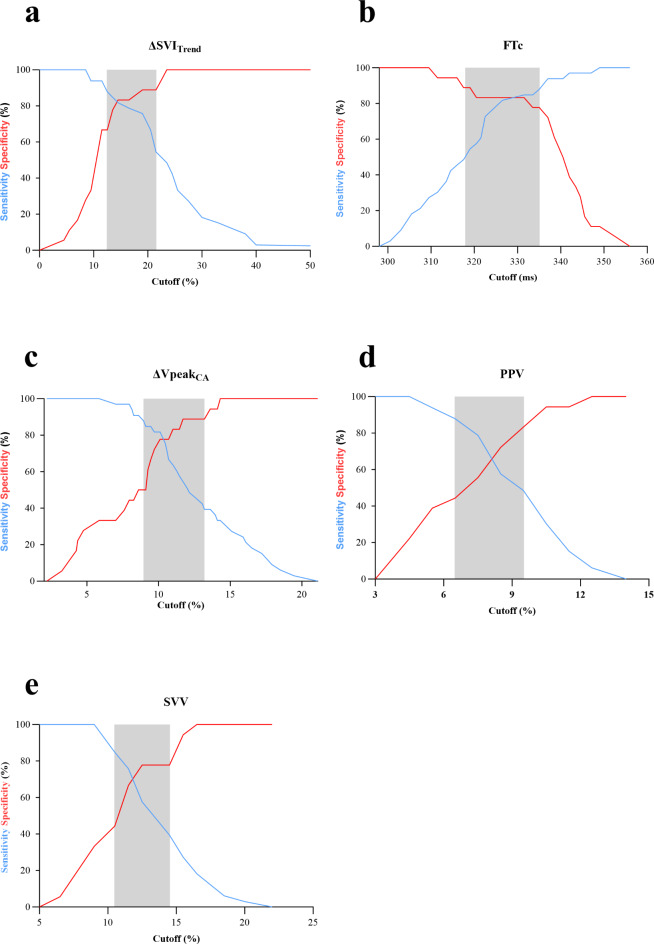
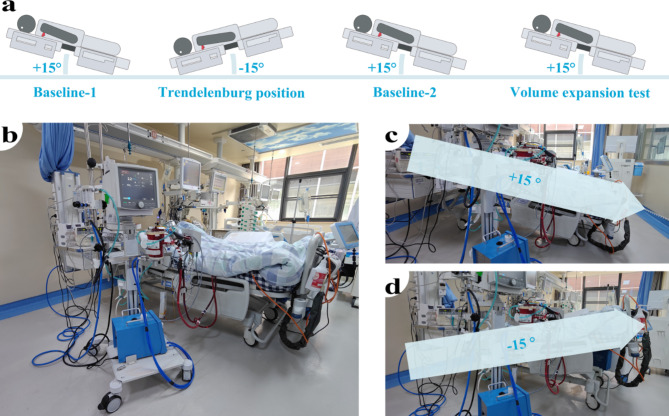
Fluid administration is widely used to treat hypotension in patients undergoing veno-venous extracorporeal membrane oxygenation (VV-ECMO). However, excessive fluid administration may lead to fluid overload can aggravate acute respiratory distress syndrome (ARDS) and increase patient mortality, predicting fluid responsiveness is of great significance for VV-ECMO patients. This prospective single-center study was conducted in a medical intensive care unit (ICU) and finally included 51 VV-ECMO patients with ARDS in the prone position (PP). Stroke volume index variation (ΔSVI), pulse pressure variation (PPV), stroke volume variation (SVV), baseline carotid corrected flow time (FTc), and respirophasic variation in carotid artery blood flow peak velocity (ΔVpeak) were taken before and after the Trendelenburg position or volume expansion. Fluid responsiveness was defined as a 15% or more increase in stroke volume index as assessed by transthoracic echocardiography after the volume expansion (VE). In our study, 33 patients (64.7%) were identified as fluid responders. Stroke volume index variation induced by the Trendelenburg position (ΔSVI), FTc, and ΔVpeak demonstrated superior predictive performance of fluid responsiveness. ΔSVI had an AUC of 0.89 (95% CI, 0.80-0.98) with an optimal threshold of 14.5% (95% CI, 12.5-21.5%), with the sensitivity and specificity were 82% (95% CI, 66-91%) and 83% (95% CI, 61-94%). FTc had an AUC of 0.87 (95% CI, 0.76-0.98) with an optimal threshold of 332ms (95% CI, 318-335ms), the sensitivity and specificity were 85% (95% CI, 69-93%) and 83% (95% CI, 61-94%), respectively. ΔVpeak showed an AUC of 0.83 (95% CI, 72-95), with a 10% optimal threshold (95% CI, 9-13%), sensitivity was 82% (95% CI, 66-91%) and specificity 78% (95% CI, 55-91%). ΔSVI, FTc and ΔVpeak could effectively predict fluid responsiveness in VV-ECMO patients with ARDS in the PP. Compared to ΔSVI and ΔVpeak, FTc is easier and more direct to acquire, and it does not require Trendelenburg position or VE, making it a more accessible and efficient option for assessing fluid responsiveness.
液体输注广泛用于治疗接受静脉-静脉体外膜肺氧合(VV-ECMO)的患者的低血压。然而,过量的液体输注可能导致液体超负荷,进而加重急性呼吸窘迫综合征(ARDS)并增加患者死亡率,因此预测液体反应性对VV-ECMO患者具有重要意义。这项前瞻性单中心研究在一个医疗重症监护病房(ICU)进行,最终纳入了51例处于俯卧位(PP)的患有ARDS的VV-ECMO患者。在头低脚高位或容量扩充前后,测量每搏量指数变异(ΔSVI)、脉压变异(PPV)、每搏量变异(SVV)、基线颈动脉校正血流时间(FTc)以及颈动脉血流峰值速度的呼吸相变异(ΔVpeak)。液体反应性定义为容量扩充(VE)后经胸超声心动图评估的每搏量指数增加15%或更多。在我们的研究中,33例患者(64.7%)被确定为液体反应者。头低脚高位引起的每搏量指数变异(ΔSVI)、FTc和ΔVpeak对液体反应性具有卓越的预测性能。ΔSVI的曲线下面积(AUC)为0.89(95%可信区间,0.80 - 0.98),最佳阈值为14.5%(95%可信区间,12.5 - 21.5%),敏感性和特异性分别为82%(95%可信区间,66 - 91%)和83%(95%可信区间,61 - 94%)。FTc的AUC为0.87(95%可信区间,0.76 - 0.98),最佳阈值为332毫秒(95%可信区间,318 - 335毫秒),敏感性和特异性分别为85%(95%可信区间,69 - 93%)和83%(95%可信区间,61 - 94%)。ΔVpeak的AUC为0.83(95%可信区间,72 - 95),最佳阈值为10%(95%可信区间,9 - 13%),敏感性为82%(95%可信区间,66 - 91%),特异性为78%(95%可信区间,55 - 91%)。ΔSVI、FTc和ΔVpeak能够有效预测处于PP的患有ARDS的VV-ECMO患者的液体反应性。与ΔSVI和ΔVpeak相比,FTc获取更容易、更直接,并且不需要头低脚高位或容量扩充,使其成为评估液体反应性更易获得且高效的选择。