Khurana Ridam, Zaheer Sufian, Ahuja Sana
Department of Pathology, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India.
Department of Pathology, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India.
Int J Surg Case Rep. 2025 Jan;126:110795. doi: 10.1016/j.ijscr.2024.110795. Epub 2024 Dec 29.
Solitary extramedullary plasmacytoma (SEP) is a rare plasma cell neoplasm, constituting around 3 % of plasma cell malignancies. SEP typically presents as a single tumor, either in bone or soft tissue, without systemic disease, and is often misdiagnosed due to its nonspecific symptoms. Diagnosis requires biopsy and extensive imaging studies to exclude multiple myeloma and other malignancies. Here, we present a case of SEP located in the hilar region, initially suspected to be a lung malignancy.
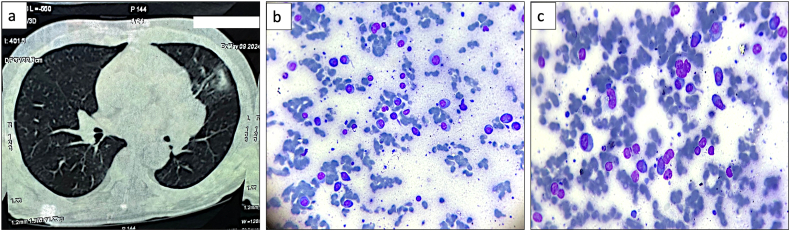
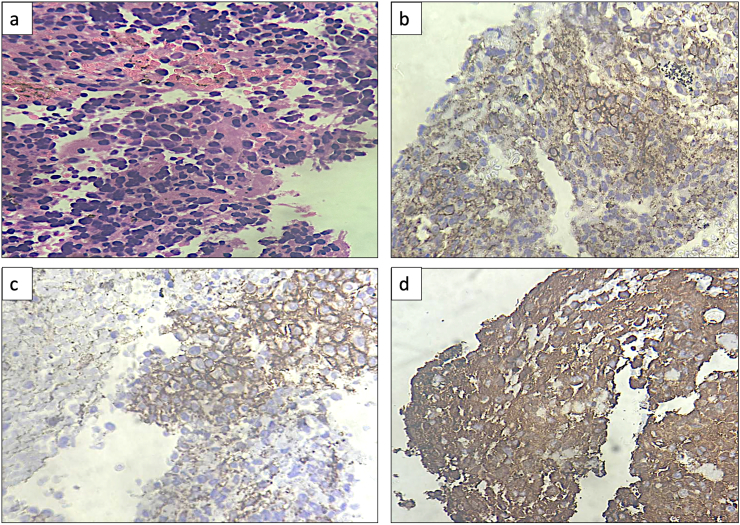
A 70-year-old male with a history of hepatitis C presented with hemoptysis and shortness of breath. PET-CT revealed a metabolically active mass in the left hilar region, encasing major vascular structures and obstructing the left upper lobe bronchus, suggesting a neoplastic process. Transbronchial biopsy showed lymphoproliferative disease, and immunohistochemistry revealed monoclonal plasma cells, confirming SEP. Laboratory tests indicated mild monoclonal gammopathy, and bone marrow aspirate showed minimal involvement with plasma cells. A diagnosis of SEP with minimal marrow involvement was made.
Extramedullary plasmacytomas are typically found in the head and neck, but rarer cases, like this one in the hilar region, may mimic lung cancer. A comprehensive diagnostic approach, including imaging, biopsy, and bone marrow analysis, is essential for accurate diagnosis and management.
This case underscores the importance of a multidisciplinary approach in diagnosing SEP, which can be easily confused with lung malignancy. Early detection and treatment, including surgery and radiotherapy, lead to favorable outcomes and reduced recurrence rates.
孤立性髓外浆细胞瘤(SEP)是一种罕见的浆细胞肿瘤,约占浆细胞恶性肿瘤的3%。SEP通常表现为单个肿瘤,可位于骨或软组织中,无全身疾病,且因其症状不具特异性常被误诊。诊断需要活检及广泛的影像学检查以排除多发性骨髓瘤和其他恶性肿瘤。在此,我们报告一例位于肺门区的SEP病例,最初怀疑为肺恶性肿瘤。
一名70岁有丙型肝炎病史的男性出现咯血和气短症状。PET-CT显示左肺门区有一个代谢活跃的肿块,包绕主要血管结构并阻塞左上叶支气管,提示为肿瘤性病变。经支气管活检显示淋巴细胞增殖性疾病,免疫组化显示单克隆浆细胞,确诊为SEP。实验室检查显示轻度单克隆丙种球蛋白病,骨髓穿刺显示浆细胞受累极少。诊断为伴有极少骨髓受累的SEP。
髓外浆细胞瘤通常见于头颈部,但像本例位于肺门区的罕见病例可能会误诊为肺癌。包括影像学、活检和骨髓分析在内的综合诊断方法对于准确诊断和治疗至关重要。
本病例强调了多学科方法在诊断SEP中的重要性,SEP很容易与肺恶性肿瘤混淆。早期检测和治疗,包括手术和放疗,可带来良好的预后并降低复发率。