Hwang Justin, Likasitwatanakul Pornlada, Deshmukh Sachin Kumar, Wu Sharon, Kwon Jason J, Toye Eamon, Moline David, Evans Mark G, Elliott Andrew, Passow Rachel, Luo Christine, John Emily, Gandhi Nishant, McKay Rana R, Heath Elisabeth I, Nabhan Chadi, Reizine Natalie, Orme Jacob J, Domingo Domenech Josep M, Sartor Oliver, Baca Sylvan C, Dehm Scott M, Antonarakis Emmanuel S
Masonic Cancer Center, University of Minnesota-Twin Cities, Minneapolis, Minnesota.
Department of Medicine, University of Minnesota-Twin Cities, Minneapolis, Minnesota.
Clin Cancer Res. 2025 Mar 3;31(5):936-948. doi: 10.1158/1078-0432.CCR-24-3471.
Around 10% to 15% of prostate cancers harbor recurrent aberrations in the Forkhead Box A1 gene, FOXA1, whereby the alteration type and the effect on the forkhead (FKH) domain affect protein function. We developed a FOXA1 classification system to inform clinical management.
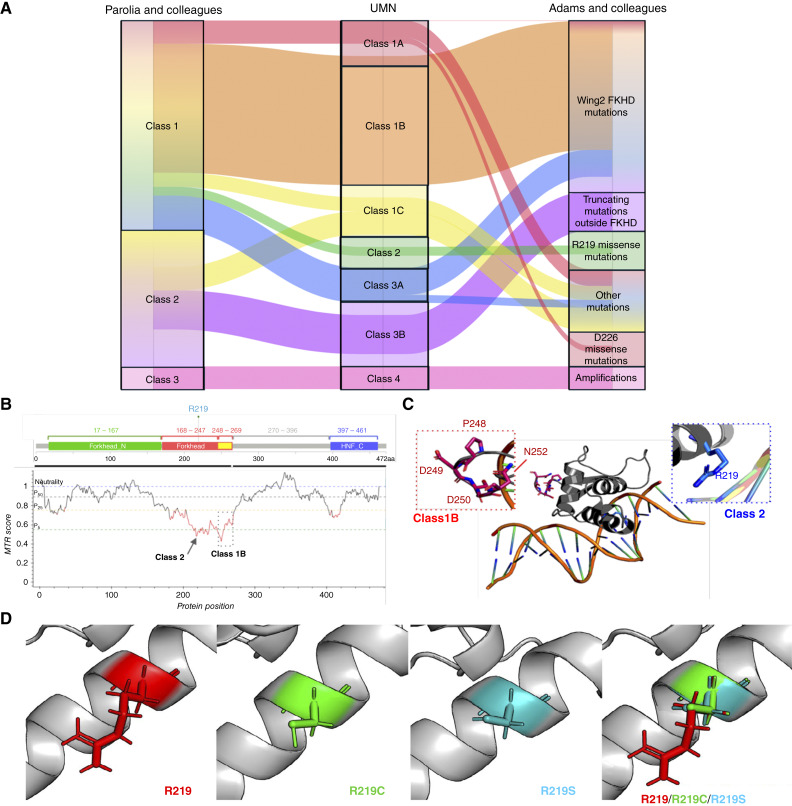
A total of 5,014 prostate cancer samples were examined using whole-exome and -transcriptome sequencing from the Caris Life Sciences database. We denoted class 1 FOXA1 alterations as missense and in-frame insertions/deletions with subclasses oriented with respect to the FKH domain. These were in the first part of the FKH domain [class 1A: amino acids (AA) 168-246], within the Wing2 region of FKH (class 1B: AA 247-269), or outside FKH (class 1C: AA 1-167, 270+). Two hotspot missense mutations at R219 were denoted class 2. Class 3 included predicted truncating mutations with subclasses partitioned based on the FKH domain (class 3A: AA 1-269 and class 3B: AA 270+). Class 4 represented FOXA1 amplifications. Real-world overall survival and therapy outcomes were determined from insurance claims.
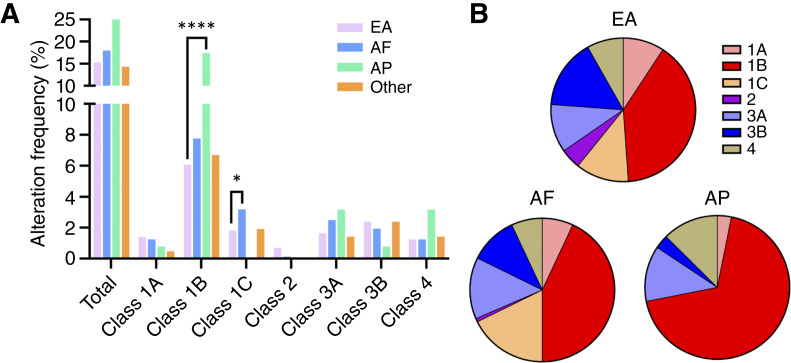
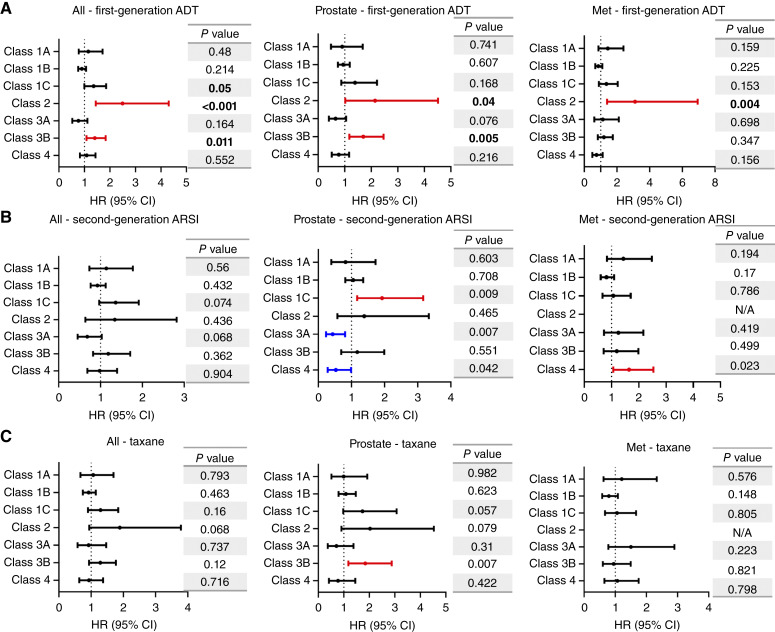
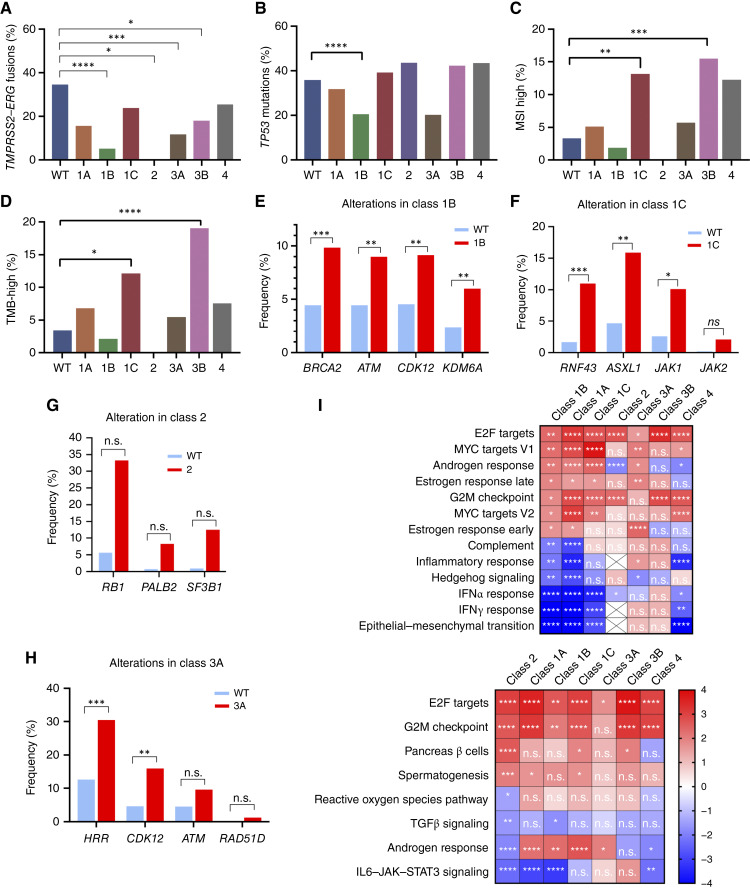
FOXA1 alterations did not influence survival when considered in aggregate but had distinct prognostic effects when stratified by class. In primary prostate samples, class 1A alterations were associated with overall improved survival (HR, 0.57; P = 0.03); a similar trend was seen in metastatic biopsies with class 1B (HR, 0.84; P = 0.09). Conversely, in primary specimens, class 1C exhibited worse survival upon second-generation androgen receptor signaling inhibitor treatment (HR, 1.93; P < 0.001). Class 2 mutations (R219C/S) were enriched in neuroendocrine prostate cancers and were associated with overall poor survival (HR, 2.05; P < 0.001) and worse outcomes to first-line androgen-deprivation therapies (HR, 2.5; P < 0.001). Class 3A alterations indicated improved survival (HR, 0.70; P = 0.01), whereas class 3B alterations portended poor outcomes (HR, 1.50; P < 0.001). Amplifications (class 4) indicated poor outcomes in metastatic samples (HR, 1.48; P = 0.02). Molecularly, different FOXA1 alteration classes harbored distinct mutational and immunologic features as well as unique transcriptional programs. Finally, relative to European Americans, African Americans had increased class 1C alterations, whereas Asian/Pacific Islander patients had increased class 1B alterations.
FOXA1 alterations should not be interpreted in aggregate, as different classes are associated with divergent molecular features and clinical outcomes. Our revised classification schema facilitates clinical decision-making for patients with prostate cancer and uncovers important racial differences.
约10%至15%的前列腺癌存在叉头框A1基因(FOXA1)的复发性畸变,其中改变类型以及对叉头(FKH)结构域的影响会影响蛋白质功能。我们开发了一种FOXA1分类系统以指导临床管理。
使用来自Caris生命科学数据库的全外显子组和转录组测序对总共5014份前列腺癌样本进行检测。我们将1类FOXA1改变定义为错义突变以及框内插入/缺失,并根据FKH结构域对亚类进行分类。这些位于FKH结构域的第一部分(1A类:氨基酸(AA)168 - 246)、FKH的Wing2区域内(1B类:AA 247 - 269)或FKH之外(1C类:AA 1 - 167、270及以上)。R219处的两个热点错义突变定义为2类。3类包括预测的截短突变,并根据FKH结构域进行亚类划分(3A类:AA 1 - 269和3B类:AA 270及以上)。4类代表FOXA1扩增。通过保险理赔确定实际的总生存期和治疗结果。
总体而言,FOXA1改变不影响生存期,但按类别分层时具有不同的预后效应。在原发性前列腺样本中,1A类改变与总体生存期改善相关(风险比[HR],0.57;P = 0.03);在转移性活检样本中,1B类也有类似趋势(HR,0.84;P = 0.09)。相反,在原发性样本中,1C类在接受第二代雄激素受体信号抑制剂治疗时生存期较差(HR,1.93;P < 0.001)。2类突变(R219C/S)在神经内分泌前列腺癌中富集,与总体生存期差相关(HR,2.05;P < 0.001),并且一线雄激素剥夺治疗效果较差(HR,2.5;P < 0.001)。3A类改变提示生存期改善(HR,0.70;P = 0.01),而3B类改变预示预后不良(HR,1.50;P < 0.001)。扩增(4类)在转移性样本中提示预后不良(HR,1.48;P = 0.02)。在分子层面,不同的FOXA1改变类别具有不同的突变和免疫特征以及独特的转录程序。最后,相对于欧裔美国人,非裔美国人的1C类改变增加,而亚裔/太平洋岛民患者的1B类改变增加。
不应将FOXA1改变作为一个整体来解释,因为不同类别与不同的分子特征和临床结果相关。我们修订的分类模式有助于前列腺癌患者的临床决策制定,并揭示了重要的种族差异。