Young Carolyn A, Chaouch Amina, Mcdermott Christopher J, Al-Chalabi Ammar, Chhetri Suresh K, Bidder Caroline, Edmonds Elizabeth, Ellis Cathy, Annadale Joe, Wilde Lisa, Sharrack Basil, Malaspina Andrea, Leach Oliver, Mills Roger, Tennant Alan
Walton Centre NHS Foundation Trust, Liverpool, UK.
University of Liverpool, Liverpool, UK.
Amyotroph Lateral Scler Frontotemporal Degener. 2025 May;26(3-4):192-202. doi: 10.1080/21678421.2024.2435969. Epub 2025 Jan 3.
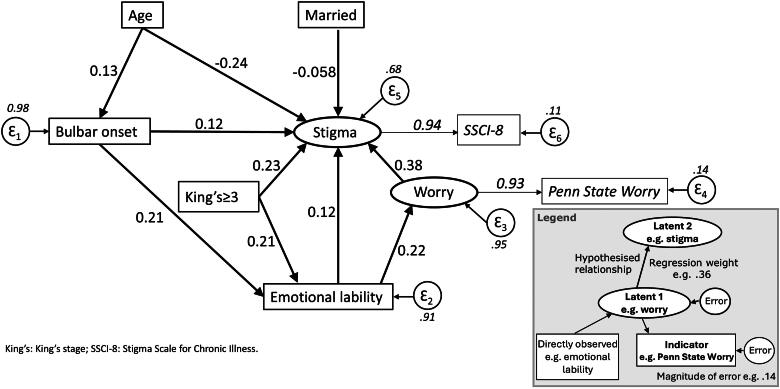
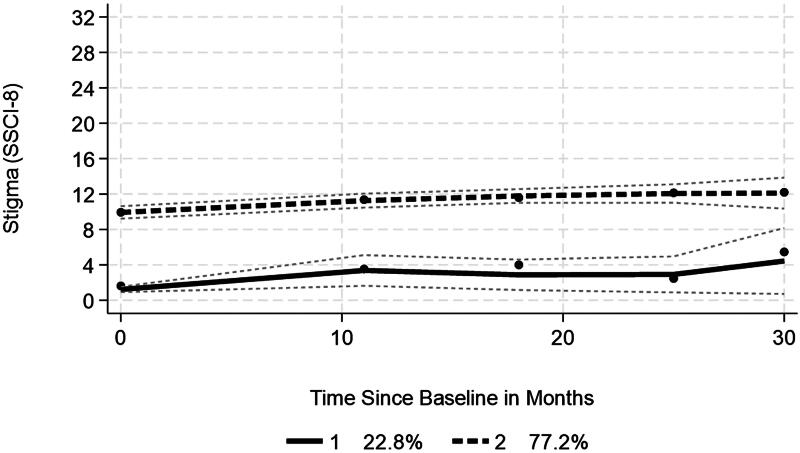
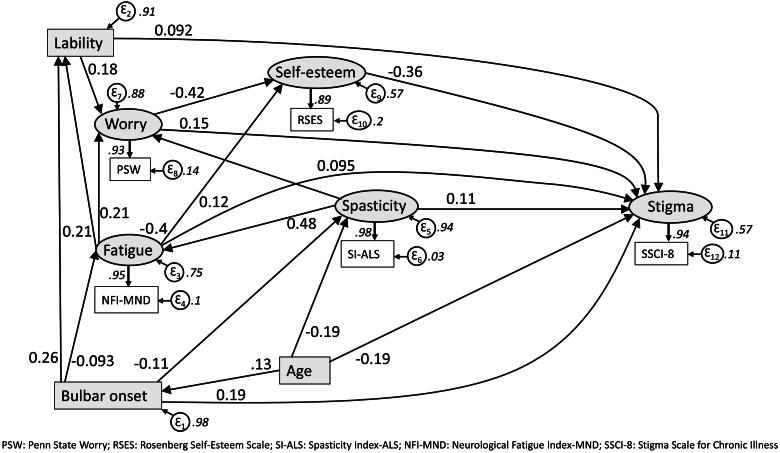
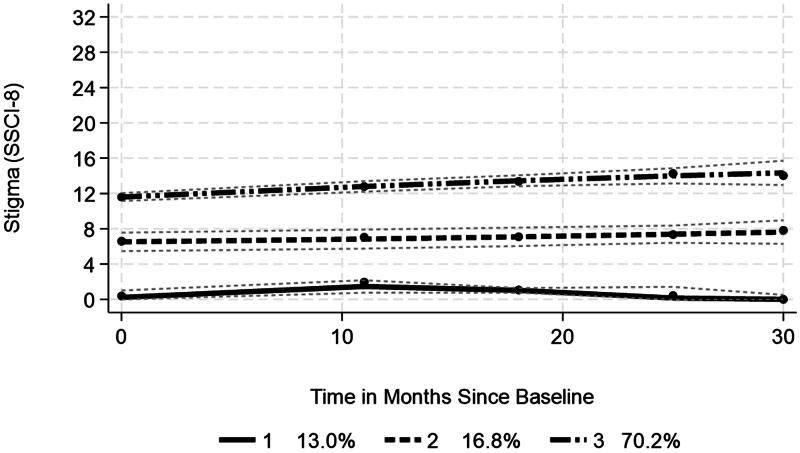
: Stigma in amyotrophic lateral sclerosis/motor neurone disease (ALS/MND) may be felt or enacted; felt stigma covers feeling devalued by the illness, whereas enacted stigma refers to being treated differently because of it. Stigma in ALS/MND has been shown to increase social withdrawal, worsen quality of life, and reduce use of assistive devices, so we explored prevalence and factors influencing stigma. : Participants in the Trajectories of Outcome in Neurological Conditions-ALS study completed scales measuring stigma, fatigue, spasticity, functioning, mood, worry, self-esteem, and perceived health, as well as demographic information and symptoms like head drop or emotional lability. Following transformation to interval-scale estimates, data were analyzed by regression, structural equation modeling, and trajectory models. : Stigma was experienced by 83.5% of 1059 respondents. Worry, disease severity (King's stage ≥ 3), emotional lability, fatigue, spasticity, and bulbar onset increase stigma. In contrast, increasing age, living with spouse/partner, and greater self-esteem were associated with reduced stigma. Trajectory analysis over 30 months ( = 1049) showed three groups, the largest (70.2%) had high levels of stigma which significantly increased during follow-up. In a recently diagnosed subset of 347 participants, stigma was experienced early in the disease course (<7 months after diagnosis), and for 77.2% stigma significantly increased over time. : Both felt and enacted stigma are frequently perceived by people living with ALS/MND. Younger people and those with bulbar onset, emotional lability, worry, fatigue, and spasticity, or at more advanced clinical stages, are at greater risk.
肌萎缩侧索硬化症/运动神经元病(ALS/MND)中的污名可能是感受到的,也可能是表现出来的;感受到的污名包括因疾病而感到自身被贬低,而表现出来的污名是指因此而受到不同的对待。研究表明,ALS/MND中的污名会增加社交退缩、恶化生活质量并减少辅助设备的使用,因此我们探讨了污名的患病率及影响因素。:神经疾病-ALS结局轨迹研究的参与者完成了测量污名、疲劳、痉挛、功能、情绪、担忧、自尊和感知健康的量表,以及人口统计学信息和诸如垂头或情绪不稳定等症状。在转换为区间尺度估计值后,通过回归分析、结构方程模型和轨迹模型对数据进行分析。:1059名受访者中有83.5%经历过污名。担忧、疾病严重程度(金斯分期≥3期)、情绪不稳定、疲劳、痉挛和延髓起病会增加污名。相比之下,年龄增长、与配偶/伴侣同住以及更高的自尊与污名减少有关。30个月(n = 1049)的轨迹分析显示有三组,最大的一组(70.2%)污名水平较高,且在随访期间显著增加。在347名参与者的最近诊断子集中,污名在疾病病程早期(诊断后<7个月)就出现了,77.2%的人污名随时间显著增加。:ALS/MND患者经常会感受到感受到的污名和表现出来的污名。年轻人以及那些延髓起病、情绪不稳定、担忧、疲劳、痉挛或处于更晚期临床阶段的人风险更大。