Sumi Toshiyuki, Nagano Yutaro, Yokoo Keiki, Ishikawa Tatsuru, Nishikiori Hirotaka, Honjo Osamu, Kudo Sayaka, Yamazoe Masami, Kondoh Shun, Shioya Makoto, Otsuka Mitsuo, Hashimoto Midori, Yabe Hayato, Tanaka Yusuke, Sudo Yuta, Yanagi Masahiro, Takahashi Mamoru, Chiba Hirofumi
Department of Pulmonary Medicine, Hakodate Goryoukaku Hospital, 38-3 Goryoukaku-Cho, Hakodate-Shi, Hokkaido, 040-8611, Japan.
Department of Respiratory Medicine and Allergology, Sapporo Medical University School of Medicine, Sapporo, Japan.
Cancer Immunol Immunother. 2025 Jan 3;74(2):39. doi: 10.1007/s00262-024-03890-4.
Compared to platinum-based therapies, a combination of ipilimumab (anti-CTLA-4) and nivolumab (anti-PD-1) has demonstrated improved outcomes in advanced non-small cell lung cancer (NSCLC), albeit with higher rates of immune-related adverse events (irAEs). This multicenter retrospective study evaluated the efficacy and safety of nivolumab and ipilimumab with or without chemotherapy (NI and NICT) in real-world clinical settings.
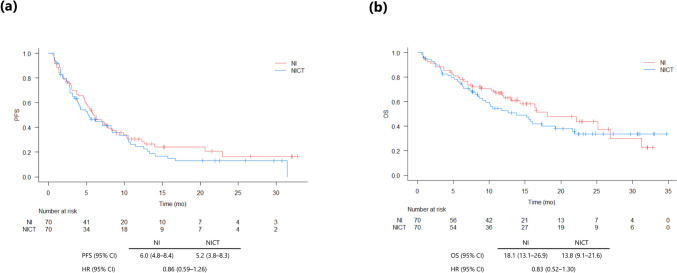
We enrolled 215 treatment-naïve NSCLC patients who received NI or NICT between December 2020 and May 2023 at 14 institutions in Japan. Severe irAEs (Grade ≥ 3) were assessed using the Common Terminology Criteria for Adverse Events. Progression-free survival (PFS) and overall survival (OS) were evaluated using Kaplan-Meier methods and propensity score matching.
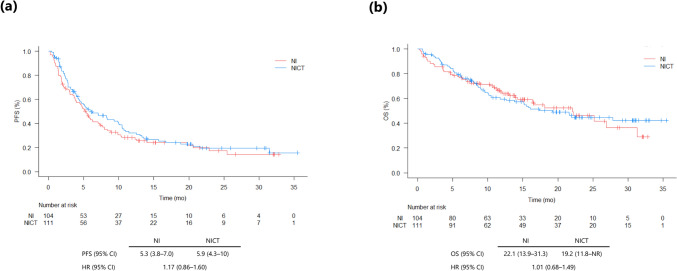
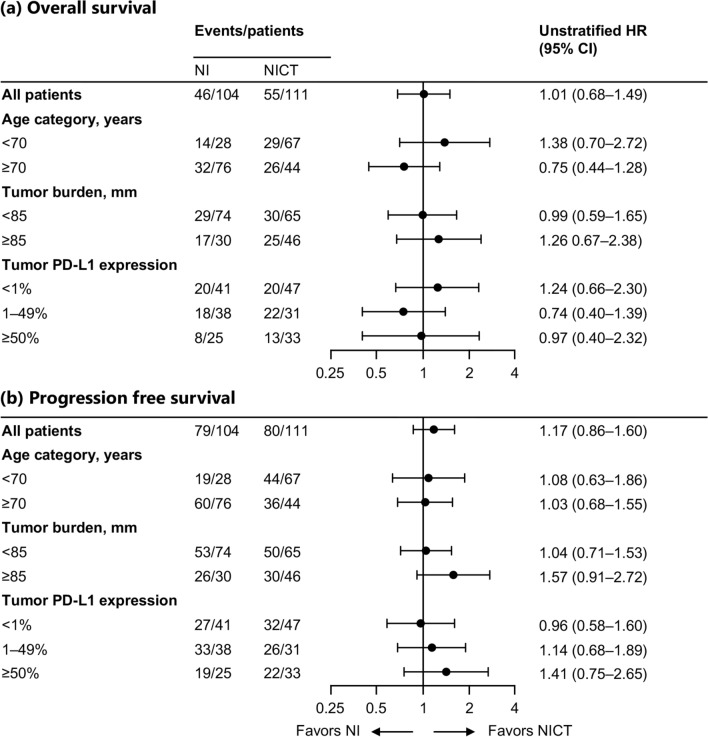
Of 215 patients, 104 and 111 received NI and NICT, respectively. The median PFS was 5.3 and 5.9 months for NI and NICT, respectively. The median OS was 22.1 and 19.2 months for NI and NICT, respectively. High fever within 3 weeks of treatment initiation and high tumor burden were indicators of severe irAEs. Grade 3 or higher irAEs occurred in 36.5% patients in the NI group and 50.5% patients in the NICT group, with higher treatment-related mortality in the NICT group (5.4% vs. 1.9% in NI).
NI and NICT showed comparable efficacies in PFS and OS. However, NICT had a higher incidence of severe irAEs and treatment-related mortality. High tumor burden and early high fever were predictors of severe irAEs. Further research is warranted to optimize the efficacy and safety of NICT for NSCLC treatment.
与铂类疗法相比,伊匹木单抗(抗CTLA-4)和纳武利尤单抗(抗PD-1)联合使用在晚期非小细胞肺癌(NSCLC)中显示出更好的疗效,尽管免疫相关不良事件(irAE)的发生率更高。这项多中心回顾性研究评估了纳武利尤单抗和伊匹木单抗联合或不联合化疗(NI和NICT)在真实临床环境中的疗效和安全性。
我们纳入了2020年12月至2023年5月期间在日本14家机构接受NI或NICT治疗的215例初治NSCLC患者。使用不良事件通用术语标准评估严重irAE(≥3级)。采用Kaplan-Meier方法和倾向评分匹配评估无进展生存期(PFS)和总生存期(OS)。
215例患者中,分别有104例和111例接受了NI和NICT治疗。NI组和NICT组的中位PFS分别为5.3个月和5.9个月。NI组和NICT组的中位OS分别为22.1个月和19.2个月。治疗开始后3周内出现高热和肿瘤负荷高是严重irAE的指标。NI组36.5%的患者和NICT组50.5%的患者发生了3级或更高等级的irAE,NICT组的治疗相关死亡率更高(5.4% vs. NI组的1.9%)。
NI和NICT在PFS和OS方面显示出相似的疗效。然而,NICT的严重irAE发生率和治疗相关死亡率更高。肿瘤负荷高和早期高热是严重irAE的预测因素。有必要进一步研究以优化NICT治疗NSCLC的疗效和安全性。