Edlow Jonathan A, Tarnutzer Alexander A
Department of Emergency Medicine, Beth Israel Deaconess Medical Center, Boston, MA, USA.
Harvard Medical School, Boston, MA, USA.
J Neurol. 2025 Jan 3;272(1):91. doi: 10.1007/s00415-024-12782-7.
Correct identification of those patients presenting with an acute vestibular syndrome (AVS) or an acute imbalance syndrome (AIS) that have underlying posterior-circulation stroke (PCS) and thus may benefit from revascularization (intravenous thrombolysis (IVT), endovascular therapy (EVT)) is important. Treatment guidelines for AVS/AIS patients are lacking. We reviewed the evidence on acute treatment strategies in AVS/AIS focusing on predictors for IVT/EVT and outcome.
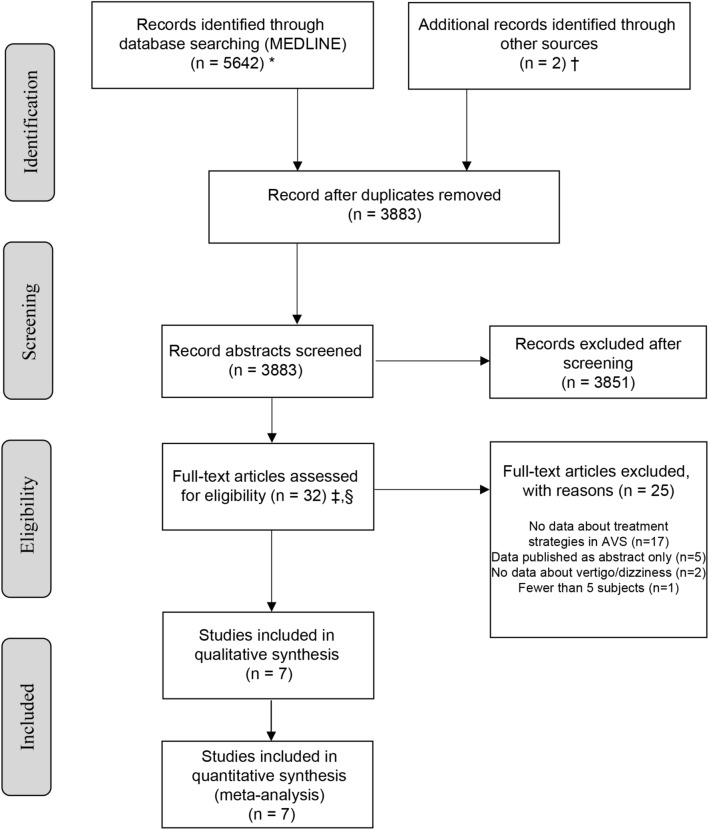
We performed a systematic search (MEDLINE, Embase) to identify studies reporting on acute treatment in PCS presenting as AVS/AIS (PROSPERO-registration = CRD42024537272). Key parameters were extracted. Risk of bias was assessed (Downs-and-Black quality assessment checklist).
We identified 3883 citations and included seven study cohorts (n = 1000 patients including 950 ischemic strokes). Overall, 251/1000 patients (25.1%) received IVT; EVT was performed in 46/368 (12.5%). Acute vertigo/dizziness was reported in 295/1000 (29.5%) patients. AVS criteria were met in 186/407 (45.7%) patients evaluated, and AIS criteria in 82/346 (23.7%). IVT was reported in 71/195 (36.4%) AVS/AIS patients and EVT in 13/77 (16.9%) cases, whereas the door-to-needle time (DNT) was significantly longer for PCS compared to anterior-circulation stroke (90 ± 29min vs. 74 ± 30min, p = 0.003) in one study. DNT was similar in those patients presenting with AVS/AIS compared to all PCS presentations in another study (70 ± 39min (AVS/AIS) vs. 63 ± 35min (all)). An mRS 2 after 90 days was noted in 68.4-69.6% of PCS. No outcome data were identified for AVS/AIS patients.
Insufficient data exist to drive any firm recommendation about treating otherwise eligible patients with AVS/AIS with IVT/EVT and judgments must be made on a case-by-case basis. Further research on this specific patient group is needed.
准确识别那些患有急性前庭综合征(AVS)或急性失衡综合征(AIS)且存在潜在后循环卒中(PCS),因而可能从血运重建(静脉溶栓(IVT)、血管内治疗(EVT))中获益的患者很重要。目前缺乏针对AVS/AIS患者的治疗指南。我们回顾了关于AVS/AIS急性治疗策略的证据,重点关注IVT/EVT的预测因素及预后。
我们进行了系统检索(MEDLINE、Embase),以识别报告以AVS/AIS形式出现的PCS急性治疗情况的研究(PROSPERO注册编号=CRD42024537272)。提取关键参数。评估偏倚风险(唐斯-布莱克质量评估清单)。
我们识别出3883条引文,并纳入了7个研究队列(n = 1000例患者,包括950例缺血性卒中)。总体而言,251/1000例患者(25.1%)接受了IVT;46/368例患者(12.5%)接受了EVT。295/1000例患者(29.5%)报告有急性眩晕/头晕。在接受评估的186/40例患者(45.7%)中符合AVS标准,82/346例患者(23.7%)符合AIS标准。71/195例AVS/AIS患者报告接受了IVT,13/77例患者(16.9%)接受了EVT,而在一项研究中,PCS患者的门到针时间(DNT)明显长于前循环卒中患者(90±29分钟对74±30分钟,p = 0.003)。在另一项研究中,与所有PCS表现的患者相比,表现为AVS/AIS的患者的DNT相似(70±39分钟(AVS/AIS)对63±35分钟(所有))。90天后改良Rankin量表(mRS)评分为2的PCS患者占68.4 - 69.6%。未找到AVS/AIS患者的预后数据。
现有数据不足以对用IVT/EVT治疗其他符合条件的AVS/AIS患者做出任何确切推荐,必须逐案做出判断。需要对这一特定患者群体进行进一步研究。