Irwan Nuradi, Takahashi Yoshiharu, Saito Kyohei, Ito Akira, Nishizawa Taketo, Sasaki Tatsuya, Faried Ahmad, Endo Toshiki
Division of Neurosurgery, Tohoku Medical and Pharmaceutical University, Sendai, Japan.
Department of Neurosurgery, Universitas Padjadjaran, Bandung, Indonesia.
J Neurosurg Case Lessons. 2025 Jan 6;9(1). doi: 10.3171/CASE24533.
The authors report the first case of thoracic interdural spinal cysts presenting as radiculopathy attributed to overdrainage-related cervical venous plexus enlargement. This case emphasizes the importance of considering interdural spinal cysts and cerebrospinal fluid overdrainage in the differential diagnosis of radiculopathy.
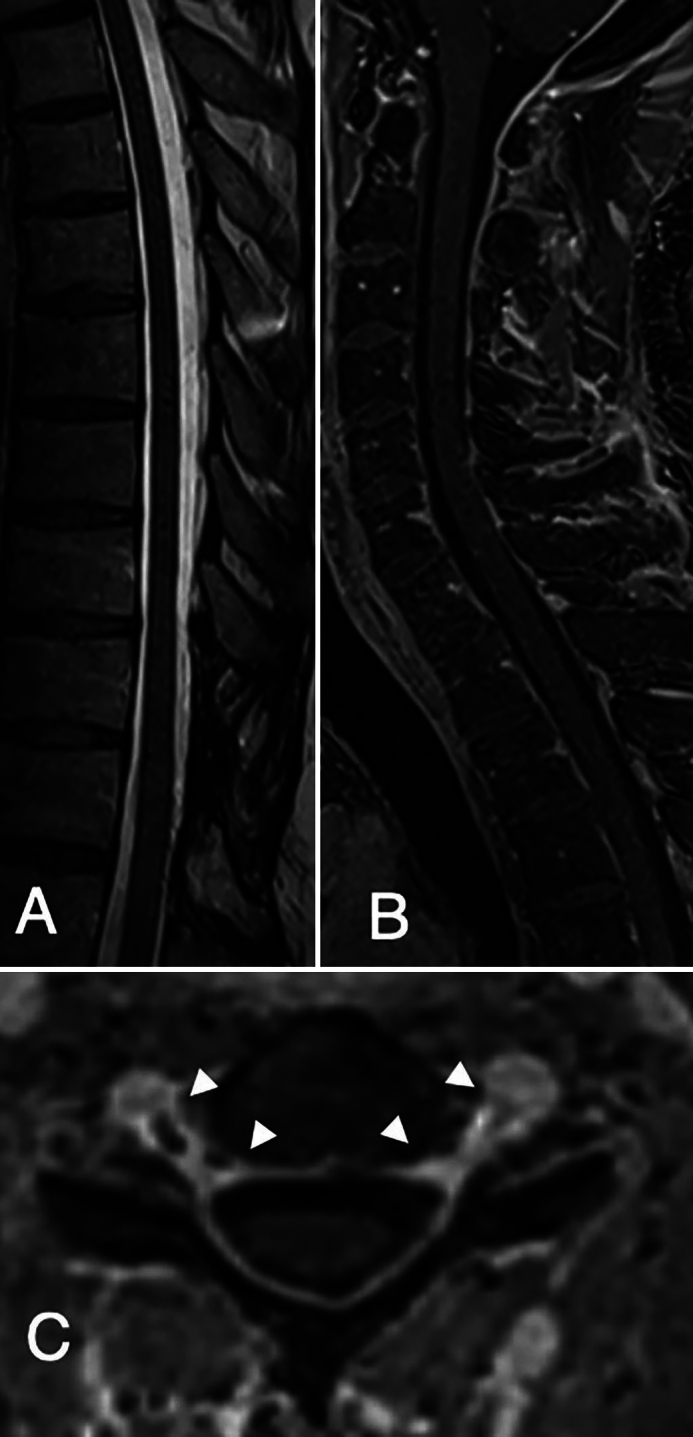
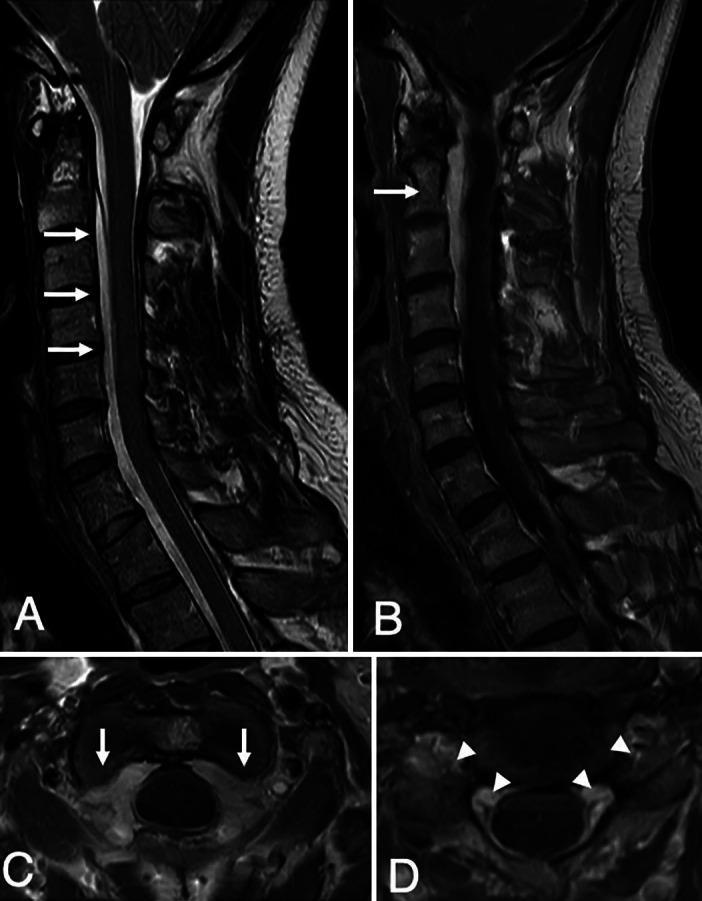
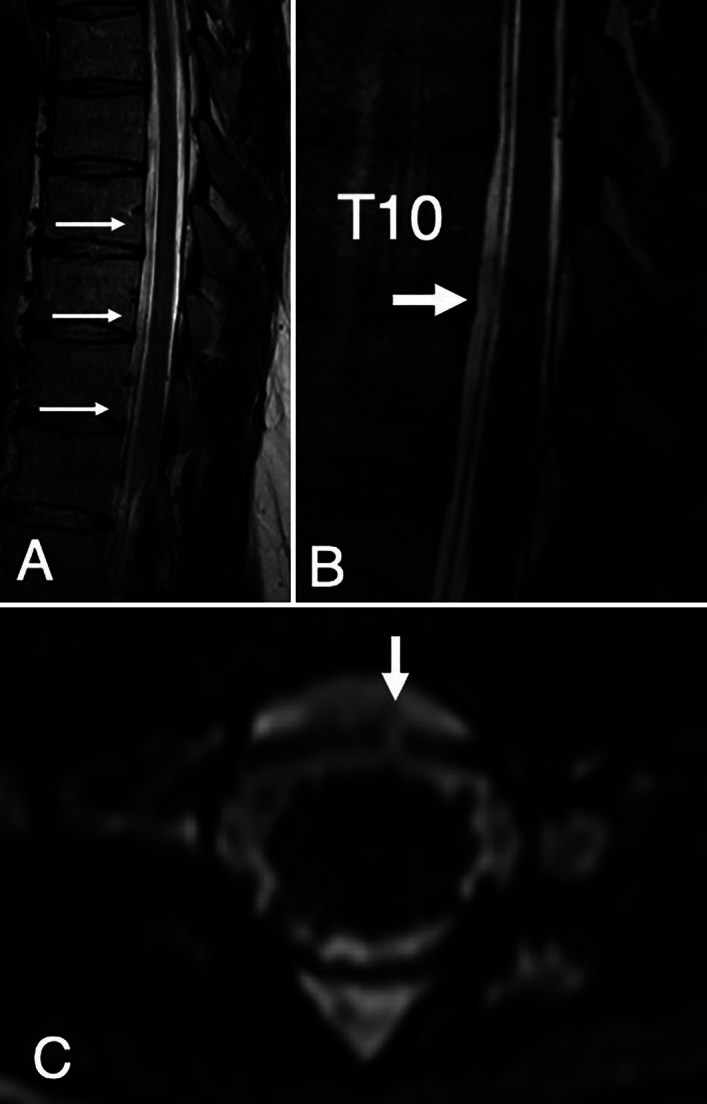
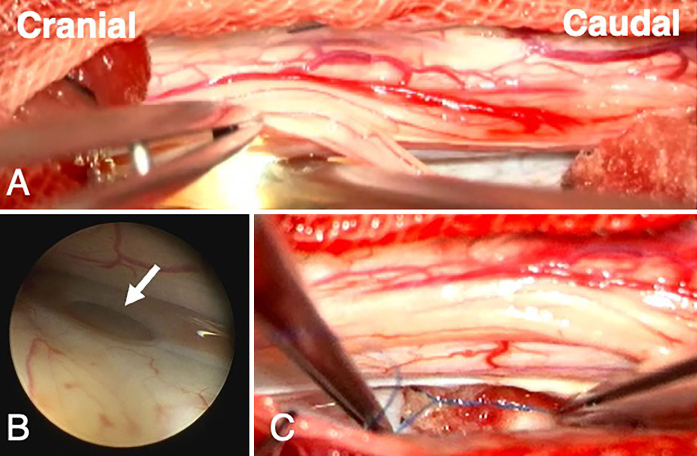
A 37-year-old male patient with a history of orthostatic headache presented with bilateral deltoid muscle atrophy consistent with C5 radiculopathy. Postcontrast magnetic resonance imaging (MRI) revealed cervical epidural venous plexus enlargement and nerve root compression. Thoracic MRI showed an interdural cyst extending from C7 to T11. In addition, a small defect in the inner layer of the dura, which connects the subarachnoid space to the cyst at the T10 level, was detected on thin-slice MRI. Surgery was performed to close the dural defect, with endoscopic assistance facilitating definitive treatment. Postoperative MRI confirmed the resolution of the spinal cyst and epidural venous enlargement. Furthermore, the patient's symptoms improved.
Evaluating the cervical spinal pathology is the common approach for cervical radiculopathy. However, in the authors' case, the presence of thoracic lesions could have been an underlying cause. Hence, identifying this unique clinical presentation can raise awareness among neurosurgeons and lead to better patient outcomes by addressing the underlying pathology in a timely manner. https://thejns.org/doi/10.3171/CASE24533.
作者报告了首例表现为神经根病的胸段硬膜间脊髓囊肿,其病因是与过度引流相关的颈静脉丛扩大。该病例强调了在神经根病鉴别诊断中考虑硬膜间脊髓囊肿和脑脊液过度引流的重要性。
一名37岁男性患者,有体位性头痛病史,出现双侧三角肌萎缩,符合C5神经根病表现。增强磁共振成像(MRI)显示颈段硬膜外静脉丛扩大和神经根受压。胸段MRI显示一个从C7延伸至T11的硬膜间囊肿。此外,在薄层MRI上检测到硬脑膜内层在T10水平有一个小缺损,该缺损将蛛网膜下腔与囊肿相连。在神经内镜辅助下进行手术封闭硬脑膜缺损,以促进确定性治疗。术后MRI证实脊髓囊肿和硬膜外静脉扩大消失。此外,患者症状改善。
评估颈段脊髓病变是诊断颈神经根病的常用方法。然而,在作者的病例中,胸段病变可能是潜在病因。因此,识别这种独特的临床表现可提高神经外科医生的认识,并通过及时处理潜在病理情况改善患者预后。https://thejns.org/doi/10.3171/CASE24533 。