Mishima S, Masuda K, Izawa Y, Mochizuki M, Namba K
Trans Am Ophthalmol Soc. 1979;77:225-79.
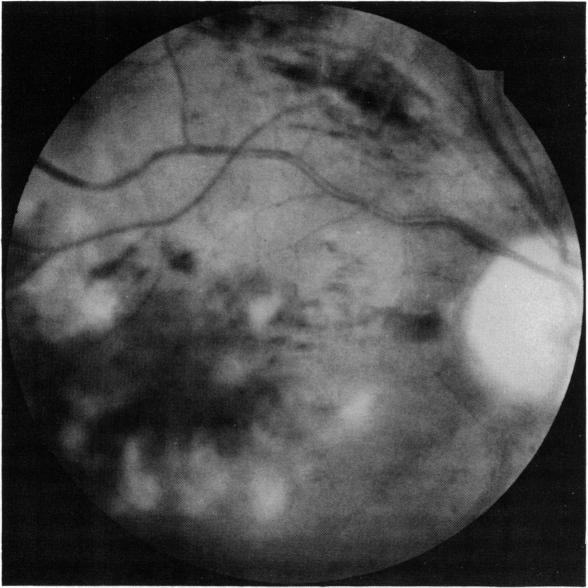
The problems of Behçet's disease in Japan have been reviewed with particular emphasis on the ophthalmologic aspects: the historical background for the Japanese works, diagnostic critieria, epidemiology, some statistics, ocular symptomatology, ocular histopathology, etiology, pathophysiology, and treatment. Behçet's disease is the most frequent entity in endogenous uveitis in Japan. Patients are found throughout the country, and the prevalence rate averages seven to eight per 100,000 population: the rate is higher in the northern than in the southern districts. The diagnosis is made on the basis of a combination of clinical symptoms that are divided into the major and minor criteria symptoms. The major criteria comprise the ocular involvement, aphthous ulcers of the oral mucous membrane, genital ulcers, and skin lesions. These symptoms recur often as attacks and the disease follows a chronic course. The ocular involvement is found in 83% to 95% in males and 67% to 73% in females; the male to female ratio in the number of patients is 1.78. Both into the anterior segment type and the fundus and panophthalmic types. The anterior segment type shows serous iridocyclitis with the classic type of hypopyon appearing in about 12% of the attacks. This type is found in about 20%, more often in females than in males, and the visual prognosis is more favorable than in the fundus and panophthalmic types. In the latter two types, attacks of retinal angitis resulting in intensive retinal edema, yellowish-white exudate, and hemorrhages recur particularly in the macular region, and the visual prognosis is poor. More than 50% of male patients lose visual acuity to less than 0.1 in five years, but this is the case in only 10% of female patients. Consequently, Behçet's disease is the cause of blindness in about 12% of acquired blindness in adults. The ocular histopathology during the attack is characterized by severe angitis with intensive infiltration of neutrophil leucocytes largely in the uveal tract and the retina; the latter is severely affected and loss of visual cells and other neural elements results. The etiology of this disease still remains unknown but genetic predisposition is suggested since this disease is strongly linked with HL-A-B5. Environmental factors are also considered. Various abnormalities are found in the blood chemistry, blood cells (particularly in neutrophil leucocytes), immunologic mechanism, fibrinolytic and blood clotting system, and hormonal system. Chemotractic factors are found in the aqueous humor. These changes are particulary enhanced just before and during the ocular attacks. Systemic corticosteroids are deleterious to the visual prognosis, but cyclophosphamide and colchicine appear to suppress attacks and help patients maintain the visual acuity. However, these drugs are toxic, particulary to the reproductive organs, and the patients must be informed of this side effect and be allowed to make a decision before they are used.

本文回顾了日本白塞病的相关问题,特别强调了眼科方面:日本研究的历史背景、诊断标准、流行病学、一些统计数据、眼部症状学、眼部组织病理学、病因、病理生理学及治疗。白塞病是日本内源性葡萄膜炎中最常见的疾病。患者遍布全国,患病率平均为每10万人中有7至8人:北部地区的患病率高于南部地区。诊断基于分为主要和次要标准症状的临床症状组合。主要标准包括眼部受累、口腔黏膜阿弗他溃疡、生殖器溃疡和皮肤病变。这些症状常反复发作,疾病呈慢性病程。男性眼部受累发生率为83%至95%,女性为67%至73%;患者数量的男女比例为1.78。眼部受累分为前段型和眼底及全眼球炎型。前段型表现为浆液性虹膜睫状体炎,约12%的发作出现典型的前房积脓。此型约占20%,女性多于男性,视力预后比眼底及全眼球炎型更有利。在后两种类型中,视网膜血管炎发作导致严重的视网膜水肿、黄白色渗出物和出血,尤其在黄斑区反复发作,视力预后较差。超过50%的男性患者在五年内视力降至0.1以下,但女性患者仅10%如此。因此,白塞病约占成人后天性失明的12%。发作期的眼部组织病理学特征为严重血管炎,中性粒细胞大量浸润,主要在葡萄膜和视网膜;视网膜严重受累,导致视细胞和其他神经成分丧失。该病病因仍不明,但由于与HL - A - B抗原强相关,提示有遗传易感性。也考虑环境因素。血液化学、血细胞(特别是中性粒细胞)、免疫机制、纤维蛋白溶解和凝血系统以及激素系统存在各种异常。房水中发现趋化因子。这些变化在眼部发作前和发作期间尤其增强。全身用皮质类固醇对视功能预后有害,但环磷酰胺和秋水仙碱似乎能抑制发作并帮助患者维持视力。然而,这些药物有毒,尤其对生殖器官,使用前必须告知患者此副作用并让其做出决定。