Mögele Tatiana, Höck Michael, Sommer Florian, Friedrich Lena, Sommer Sebastian, Schmutz Maximilian, Altenburger Amadeus, Messmann Helmut, Anthuber Matthias, Kröncke Thomas, Stüben Georg, Trepel Martin, Märkl Bruno, Dintner Sebastian, Claus Rainer
Pathology, Faculty of Medicine, University of Augsburg, 86156 Augsburg, Germany.
Bavarian Cancer Research Center (BZKF), Germany.
Cancers (Basel). 2024 Dec 14;16(24):4173. doi: 10.3390/cancers16244173.
BACKGROUND/OBJECTIVES: Locally advanced rectal cancer is treated with neoadjuvant chemoradiotherapy (nCRT) followed by total mesorectal excision (TME). As this approach achieves complete pathologic remissions (pCR) in approximately 30% of patients, it raises the question of whether surgery is always necessary. Non-surgical strategies, such as "watch and wait" (W&W), have shown similarly promising outcomes. However, there is an unmet need for reliable biomarkers predicting pCR. Analysis of circulating tumor DNA (ctDNA) has shown potential for monitoring treatment response and detecting minimal residual disease. We hypothesized that monitoring ctDNA changes during nCRT might facilitate the identification of individuals who achieve pCR.
In the prospective single-center NEORECT trial, the plasma of forty rectal cancer patients was collected before, during, and after nCRT and before TME. Informative somatic mutations were identified in tissue biopsies by NGS and subsequently used for ctDNA quantification by dPCR.
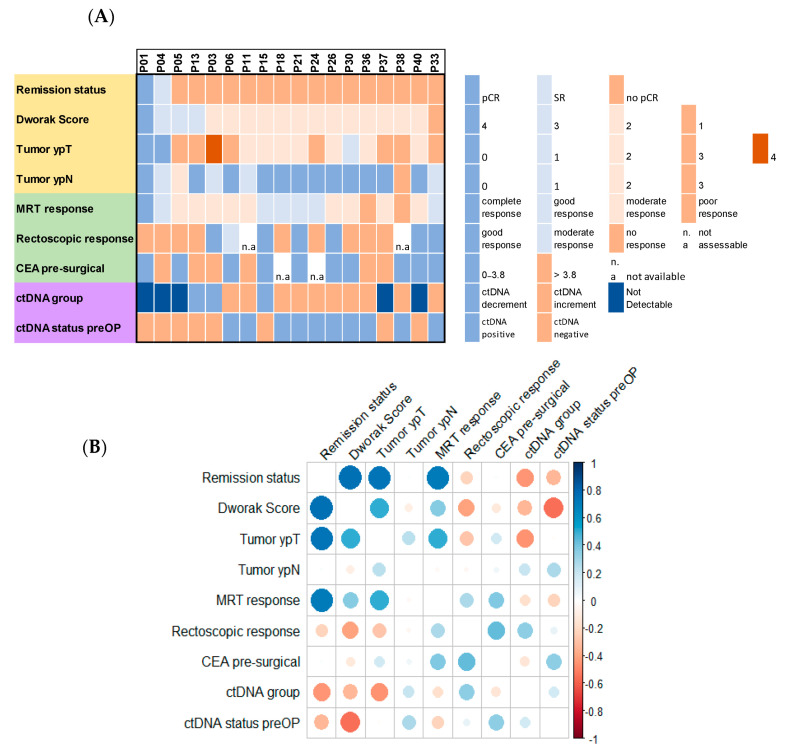
The results identified three distinct ctDNA patterns: increase, decrease, and absence. Remarkably, undetectable DNA was observed in good responders, while a tenfold ctDNA increase was associated with the emergence of new metastases. Despite these insights, ctDNA alone demonstrated low specificity, with no significant correlation to pCR or long-term prognosis. A multimodal approach incorporating routinely available clinical parameters remains inadequate for accurately predicting pCR prior to TME.
In conclusion, the NEORECT trial establishes the feasibility of ctDNA-based personalized monitoring for rectal cancer patients undergoing nCRT. However, the utility of ctDNA in enhancing pCR prediction for a W&W strategy warrants further investigation. Larger studies integrating multi-gene analyses and expanded clinical datasets are essential in the future.
背景/目的:局部晚期直肠癌采用新辅助放化疗(nCRT)后行全直肠系膜切除术(TME)进行治疗。由于这种方法在约30%的患者中实现了完全病理缓解(pCR),因此引发了是否总是需要手术的问题。非手术策略,如“观察等待”(W&W),已显示出同样有前景的结果。然而,对于预测pCR的可靠生物标志物仍有未满足的需求。循环肿瘤DNA(ctDNA)分析已显示出监测治疗反应和检测微小残留病的潜力。我们假设在nCRT期间监测ctDNA变化可能有助于识别实现pCR的个体。
在一项前瞻性单中心NEORECT试验中,在nCRT前、期间、之后以及TME前收集了40例直肠癌患者的血浆。通过二代测序(NGS)在组织活检中鉴定出信息性体细胞突变,随后用于通过数字PCR(dPCR)进行ctDNA定量。
结果确定了三种不同的ctDNA模式:增加、减少和不存在。值得注意的是,在反应良好的患者中观察到不可检测的DNA,而ctDNA增加10倍与新转移灶的出现相关。尽管有这些发现,但单独的ctDNA显示出低特异性,与pCR或长期预后无显著相关性。纳入常规可用临床参数的多模式方法在TME前准确预测pCR方面仍然不足。
总之,NEORECT试验确立了对接受nCRT的直肠癌患者进行基于ctDNA的个性化监测的可行性。然而,ctDNA在增强W&W策略的pCR预测中的效用值得进一步研究。未来整合多基因分析和扩大临床数据集的更大规模研究至关重要。