Perlova Ksenia, Schmidt Claudia C, Fink Gereon R, Weiss Peter H
Department of Neurology, Faculty of Medicine and University Hospital Cologne, University of Cologne, Kerpener Str. 62, 50937, Cologne, Germany.
Cognitive Neuroscience, Institute of Neuroscience and Medicine (INM-3), Research Centre Jülich, Leo-Brandt-Str. 5, 52425, Jülich, Germany.
Neurol Res Pract. 2025 Jan 9;7(1):2. doi: 10.1186/s42466-024-00359-8.
Apraxia is a motor-cognitive disorder that primary sensorimotor deficits cannot solely explain. Previous research in stroke patients has focused on damage to the fronto-parietal praxis networks in the left hemisphere (LH) as the cause of apraxic deficits. In contrast, the potential role of the (left) primary motor cortex (M1) has largely been neglected. However, recent brain stimulation and lesion-mapping studies suggest an involvement of left M1 in motor cognitive processes-over and above its role in motor execution. Therefore, this study explored whether the left M1 plays a specific role in apraxia.
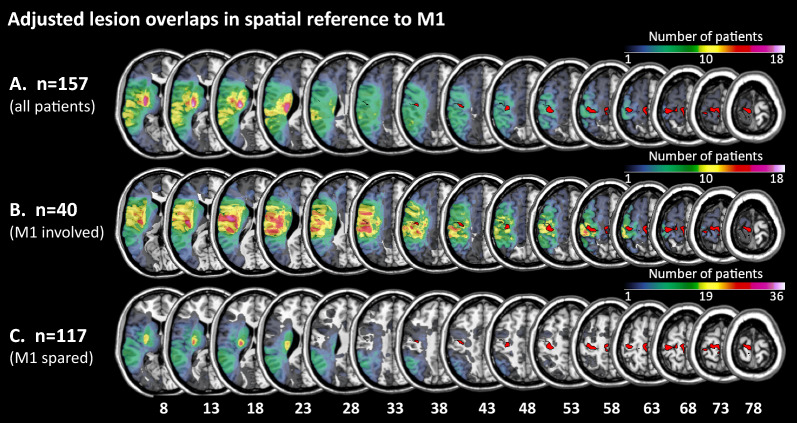
We identified 157 right-handed patients with first-ever unilateral LH stroke in the sub-acute phase (< 90 days post-stroke), for whom apraxia assessments performed with the ipsilesional left hand and lesion maps were available. Utilizing the maximum probability map of Brodmann area 4 (representing M1) provided by the JuBrain Anatomy Toolbox in SPM, patients were subdivided into two groups depending on whether their lesions involved (n = 40) or spared (n = 117) left M1. We applied a mixed model ANCOVA with repeated measures to compare apraxic deficits between the two patient groups, considering the factors "body part" and "gesture meaning". Furthermore, we explored potential differential effects of the anterior (4a) and posterior (4p) parts of Brodmann area 4 by correlation analyses.
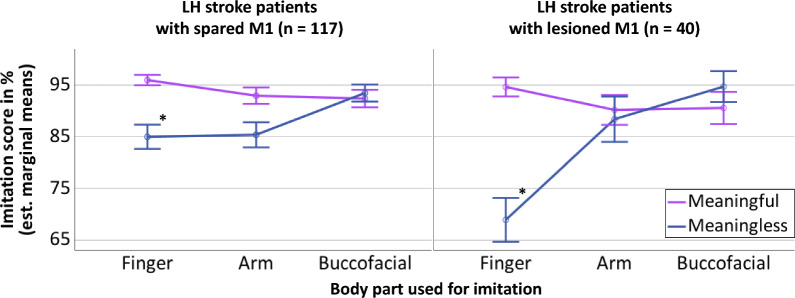
Patients with and without M1 involvement did not differ in age and time post-stroke but in lesion size. When controlling for lesion size, the total apraxia scores did not differ significantly between groups. However, the mixed model ANCOVA showed that LH stroke patients with lesions involving left M1 performed differentially worse when imitating meaningless finger gestures. This effect was primarily driven by lesions affecting Brodmann area 4p.
Even though many current definitions of apraxia disregard a relevant role of (left) M1, the observed differential effect of M1 lesions, specifically involving subarea 4p, on the imitation of meaningless finger gestures in the current sample of LH stroke patients suggests a specific role of left M1 in imitation when high amounts of (motor) attention and sensorimotor integration are required.
失用症是一种运动认知障碍,主要的感觉运动缺陷无法完全解释该障碍。先前针对中风患者的研究主要关注左半球额顶叶运用网络受损是导致失用症缺陷的原因。相比之下,(左侧)初级运动皮层(M1)的潜在作用在很大程度上被忽视了。然而,最近的脑刺激和病变图谱研究表明,除了其在运动执行中的作用外,左侧M1还参与运动认知过程。因此,本研究探讨了左侧M1在失用症中是否发挥特定作用。
我们纳入了157例首次发生单侧左半球中风的亚急性期(中风后<90天)右利手患者,这些患者均进行了患侧左手的失用症评估且有病变图谱。利用SPM中JuBrain解剖工具箱提供的布罗德曼4区(代表M1)的最大概率图,根据病变是否累及左侧M1(n = 40)或未累及(n = 117)将患者分为两组。我们应用重复测量的混合模型协方差分析来比较两组患者的失用症缺陷,考虑“身体部位”和“手势意义”因素。此外,我们通过相关性分析探讨了布罗德曼4区前部(4a)和后部(4p)的潜在差异效应。
有和没有M1受累的患者在年龄和中风后时间上无差异,但在病变大小上有差异。在控制病变大小后,两组的总失用症评分无显著差异。然而,混合模型协方差分析显示,病变累及左侧M1的左半球中风患者在模仿无意义手指手势时表现明显更差。这种效应主要由影响布罗德曼4p区的病变驱动。
尽管目前许多失用症的定义都忽略了(左侧)M1的相关作用,但在当前左半球中风患者样本中观察到的M1病变,特别是涉及4p亚区的病变,对无意义手指手势模仿的差异效应表明,在需要大量(运动)注意力和感觉运动整合时,左侧M1在模仿中发挥特定作用。