White Kyle C, Costa-Pinto Rahul, Chaba Anis, McIlroy Philippa, Senthuran Siva, Luke Stephen, Attokaran Antony G, Garrett Peter, Ramanan Mahesh, Tabah Alexis, Shekar Kiran, Laupland Kevin B, White Hayden, McCullough James, Udy Andrew, Eastwood Glenn, Bellomo Rinaldo
Intensive Care Unit, Princess Alexandra Hospital, 199 Ipswich Road, Woolloongabba, Brisbane, QLD, 4102, Australia.
Faculty of Medicine, University of Queensland, Brisbane, QLD, Australia.
Crit Care Resusc. 2024 Nov 22;26(4):295-302. doi: 10.1016/j.ccrj.2024.09.002. eCollection 2024 Dec.
The optimal timing of vasopressin initiation as an adjunctive vasopressor remains unclear. We aimed to study the association between the timing of vasopressin commencement, pre-specified physiological parameters, and hospital mortality.
We conducted a multicentre, retrospective, observational study.
Twelve ICUs in Queensland, Australia between January 2015 and December 2021.
Adult patients with septic shock who received vasopressin as an adjunctive vasopressor within 72 hours of ICU admission.
Hospital mortality.
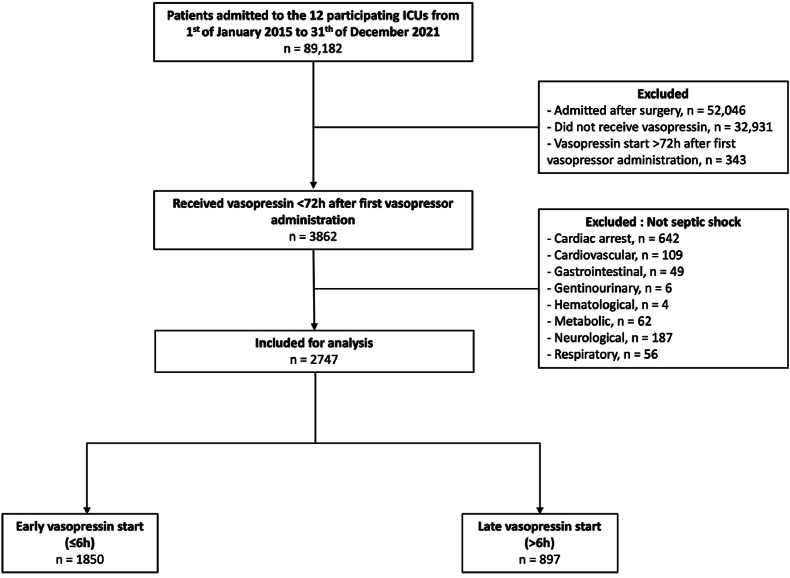
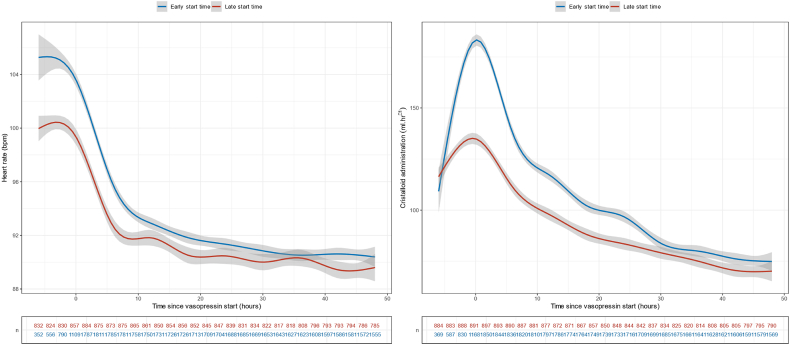
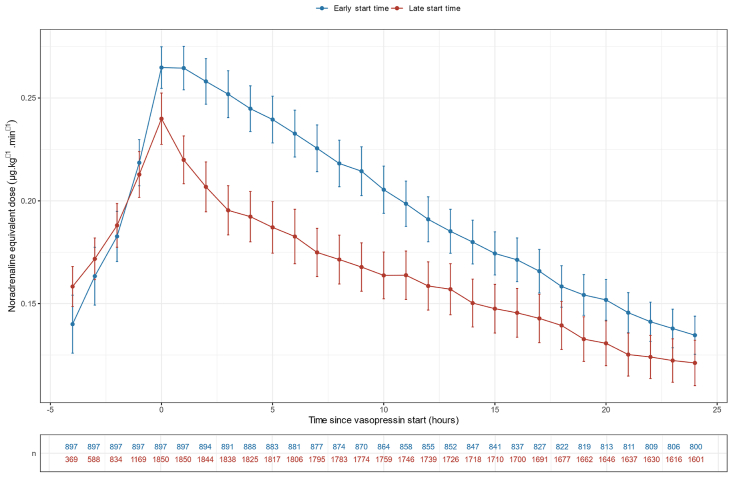
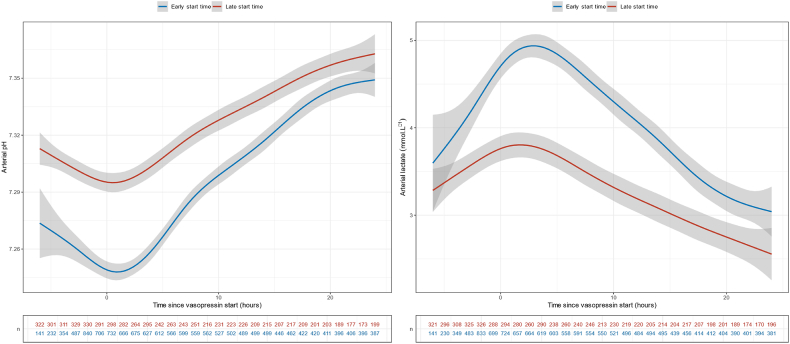
Overall, 2747 patients fulfilled the inclusion criteria. Of these, 1850 (67%) started vasopressin within six hours of vasopressor therapy start, while 897 (33%) started vasopressin between six hours and 72 hours. APACHE III score, peak lactate, and creatinine were higher in the early start group. Early vasopressin start was independently associated with decreased hospital mortality (aOR = 0.69, 95% CI = 0.57-0.83). Vasopressin infusion start was also associated with an immediate decrease in the noradrenaline-equivalent dose regardless of timing. There was a statistically significant favourable breakpoint at vasopressin start for the course of arterial pH, lactate, heart rate and crystalloid infusion rate (p<0.001).
In patients with septic shock, early adjunctive vasopressin initiation was independently associated with lower hospital mortality. Vasopressin starting at any time was also associated with reduced tachycardia, acidosis, and hyperlactatemia.
血管加压素作为辅助血管升压药开始使用的最佳时机仍不明确。我们旨在研究血管加压素开始使用的时机、预先设定的生理参数与医院死亡率之间的关联。
我们进行了一项多中心、回顾性观察研究。
2015年1月至2021年12月期间澳大利亚昆士兰州的12个重症监护病房。
入住重症监护病房72小时内接受血管加压素作为辅助血管升压药的成年感染性休克患者。
医院死亡率。
总体而言,2747例患者符合纳入标准。其中,1850例(67%)在血管升压药治疗开始后6小时内开始使用血管加压素,而897例(33%)在6小时至72小时之间开始使用血管加压素。早期开始组的急性生理与慢性健康状况评分系统III(APACHE III)评分、乳酸峰值和肌酐水平更高。早期使用血管加压素与降低医院死亡率独立相关(校正比值比[aOR]=0.69,95%置信区间[CI]=0.57-0.83)。无论时机如何,血管加压素输注开始也与去甲肾上腺素等效剂量的立即降低相关。在血管加压素开始使用时,动脉pH值、乳酸、心率和晶体液输注速率的变化过程存在统计学上显著的有利断点(p<0.001)。
在感染性休克患者中,早期辅助使用血管加压素与较低的医院死亡率独立相关。在任何时间开始使用血管加压素也与心动过速、酸中毒和高乳酸血症的减轻相关。