Melchers Max, de Smet Vivienne, Rooijakkers Chrissie, Huising Jonathan, Vermeulen Wander, Köktaş Beyza Nur Nisa, van de Vusse Karlijn Johanna, Sabzewar Kimia Milani, Mishra Shakti Bedanta, Bethlehem Carina, Boer Dirk P, Cimic Nedim, van Duijnhoven Mirella, Frenzel Tim, Liesveld Jordi, Paternoster Gianluca, Stads Susanne, Weenink Jan J, Festen-Spanjer Barbara, Pickkers Peter, van Zanten Arthur Raymond Hubert
Department of Intensive Care, Gelderse Vallei Hospital, Ede, the Netherlands.
Division of Human Nutrition and Health, Wageningen University & Research, Wageningen, the Netherlands.
Ann Intensive Care. 2025 Apr 29;15(1):59. doi: 10.1186/s13613-025-01472-w.
The Surviving Sepsis Campaign guidelines suggest adding arginine vasopressin (AVP) when norepinephrine (NE) doses reach 0.25-0.50 µg/kg/min in septic shock patients. However, relying solely on a NE threshold has limitations, as other factors may be valuable in guiding AVP therapy during septic shock. Therefore, we aimed to identify additional patient characteristics associated with AVP hemodynamic responsiveness.
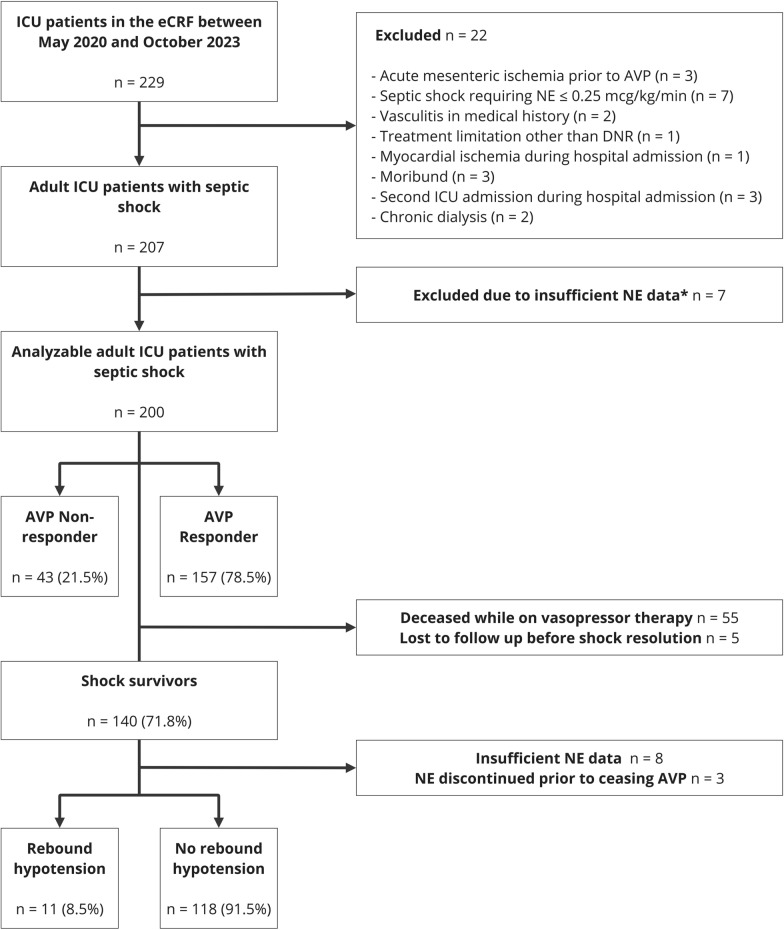
A multicenter, prospective, observational study was conducted among adult ICU patients who met the predefined criteria for septic shock (not reaching the individual target mean arterial pressure despite adequate fluid resuscitation and NE base dose > 0.25 µg/kg/min) and received AVP therapy. AVP hemodynamic responsiveness was the primary study outcome, defined as stabilization or decrease of NE infusion rate two hours after initiating AVP. Secondary outcomes included shock duration and rebound hypotension following termination of AVP infusion. Univariate and multivariable regression analyses were performed to detect associations between characteristics and outcomes.
Between May 2020 and October 2023, 200 septic shock patients originating from 11 different ICUs were included. Of these, 153 (79%) met the definition for AVP hemodynamic responsiveness. Obesity and hyperlactatemia was negatively associated with AVP-response (adjusted Odds Ratio [aOR] 0.30, 95%CI 0.14-0.65 and aOR 0.86, 95%CI 0.75-0.99, respectively), while a NE infusion rate ≥ 0.30 µg/kg/min showed positive odds of AVP response (aOR 2.33, 95%CI 1.06-5.14). Incidence of new-onset atrial fibrillation was lower in AVP responders than non-responders (4% vs. 14%, p = 0.013). Higher body mass index (BMI) , NE infusion rate and duration prior to AVP initiation was associated with longer shock duration (aOR 1.06, 95%CI 1.02-1.11, aOR 1.12, 95%CI 1.01-1.25, and 1.01 95% CI 1.00-1.03, respectively), while higher pH associated with lower likelihood of prolonged shock (aOR 0.80, 95%CI 0.64-0.99). Rebound hypotension occurred in 9% when AVP was terminated, and AVP duration > 24 h was negatively associated with rebound hypotension (OR 0.22, 95%CI 0.05-0.85).
Arterial lactate, pH, BMI, and NE duration and dose were associated with AVP responsiveness and shock duration during septic shock, and rebound hypotension occurred in 9% during recovery. Our findings suggest that beyond NE thresholds, specific factors could be considered to optimize adjunctive AVP therapy in septic shock patients.
拯救脓毒症运动指南建议,对于脓毒性休克患者,当去甲肾上腺素(NE)剂量达到0.25 - 0.50微克/千克/分钟时,加用精氨酸加压素(AVP)。然而,单纯依赖NE阈值存在局限性,因为在脓毒性休克期间,其他因素可能对指导AVP治疗有价值。因此,我们旨在确定与AVP血流动力学反应相关的其他患者特征。
对符合脓毒性休克预定义标准(尽管进行了充分的液体复苏且NE基础剂量>0.25微克/千克/分钟,但未达到个体目标平均动脉压)并接受AVP治疗的成年ICU患者进行了一项多中心、前瞻性、观察性研究。AVP血流动力学反应是主要研究结局,定义为开始使用AVP两小时后NE输注速率稳定或降低。次要结局包括休克持续时间和停止AVP输注后的反弹性低血压。进行单变量和多变量回归分析以检测特征与结局之间的关联。
在2020年5月至2023年10月期间,纳入了来自11个不同ICU的200例脓毒性休克患者。其中,153例(79%)符合AVP血流动力学反应的定义。肥胖和高乳酸血症与AVP反应呈负相关(调整后的优势比[aOR]分别为0.30,95%置信区间0.14 - 0.65和aOR 0.86,95%置信区间0.75 - 0.99),而NE输注速率≥0.30微克/千克/分钟显示出AVP反应的正优势(aOR 2.33,95%置信区间1.06 - 5.14)。AVP反应者中新发房颤的发生率低于无反应者(4%对14%,p = 0.013)。较高的体重指数(BMI)、NE输注速率和开始使用AVP前的持续时间与较长的休克持续时间相关(aOR分别为1.06,95%置信区间1.02 - 1.11;aOR 1.12,95%置信区间1.01 - 1.25;以及1.01,95%置信区间1.00 - 1.03),而较高的pH值与休克延长的可能性较低相关(aOR 0.80,95%置信区间0.64 - 0.99)。停止AVP时,9%的患者发生反弹性低血压,AVP持续时间>24小时与反弹性低血压呈负相关(优势比0.22,95%置信区间0.05 - 0.85)。
动脉血乳酸、pH值、BMI以及NE持续时间和剂量与脓毒性休克期间的AVP反应性和休克持续时间相关,恢复期间9%的患者发生反弹性低血压。我们的研究结果表明,除了NE阈值外,还可以考虑特定因素来优化脓毒性休克患者的辅助AVP治疗。