Alnughmush Ahmed, Sayyed Ayman, Remberger Mats, Al-Shaibani Eshrak, Chen Carol, Chiarello Caden, Pasic Ivan, Novitzky-Basso Igor, Law Arjun Datt, Lam Wilson, Kim Dennis Dong Hwan, Gerbitz Armin, Viswabandya Auro, Kumar Rajat, Michelis Fotios V, Mattsson Jonas
Department of Medicine, University of Toronto, Toronto, ON, Canada.
Hans Messner Allogeneic Transplant Program, Division of Medical Oncology and Hematology, Princess Margaret Cancer Centre, University Health Network, Toronto, ON, Canada.
Transplant Direct. 2025 Jan 9;11(2):e1753. doi: 10.1097/TXD.0000000000001753. eCollection 2025 Feb.
Despite decades of post-allogeneic hematopoietic cell transplantation (HCT) growth factor utilization, its role remains undefined, leading to ongoing debates and research. The theoretical impacts of growth factors have been challenged in numerous studies.
In this retrospective cohort study conducted at the Princess Margaret Cancer Centre, we analyzed the clinical outcomes of 509 patients who underwent allogeneic HCT between May 1, 2019, and May 31, 2022. This study aimed to assess the impact of granulocyte colony-stimulating factor (G-CSF) administration posttransplantation on neutrophil and platelet engraftment, incidence of bloodstream infections (BSIs), graft-versus-host disease, engraftment syndrome (ES), and survival metrics including overall survival, nonrelapse mortality, and graft-versus-host disease-free/relapse-free survival.
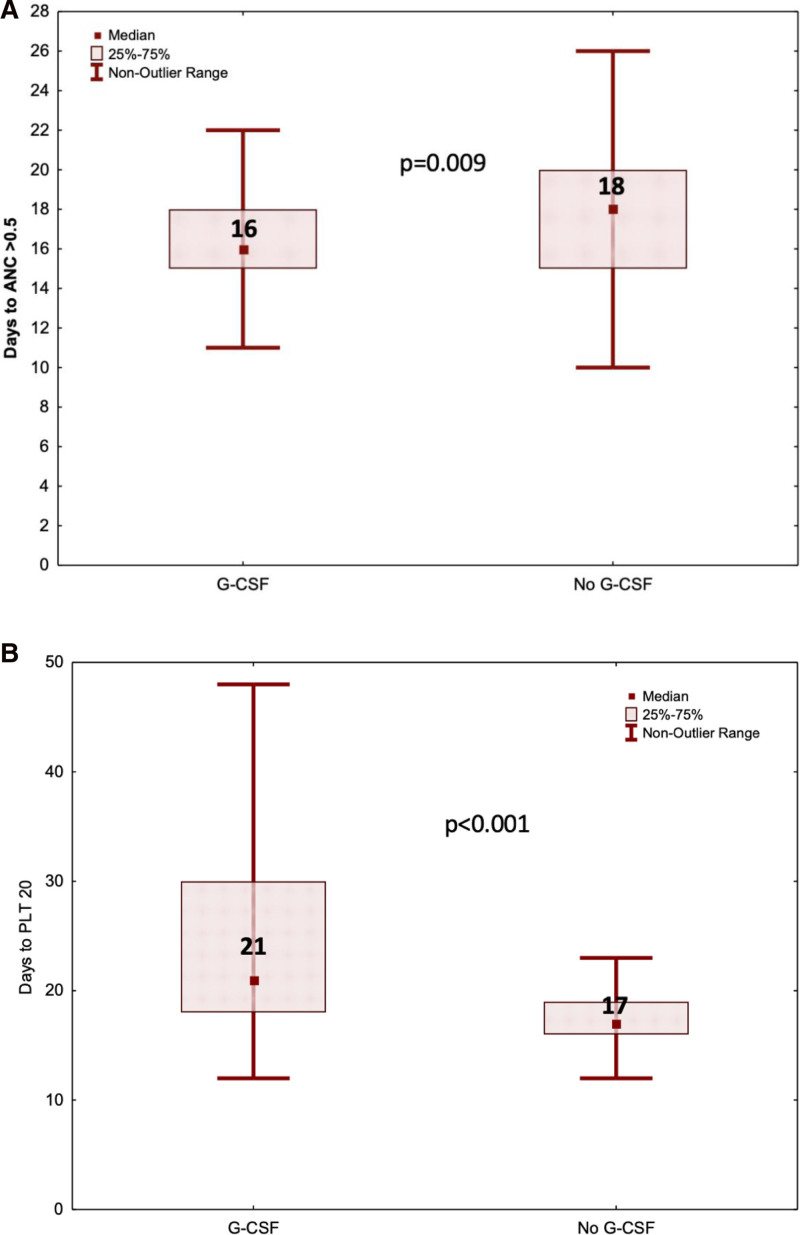
Our findings indicate that G-CSF administration expedited neutrophil engraftment (16 versus 18 d, = 0.009) and was associated with a decreased incidence of BSI (9.4% versus 31.3%, = 0.014). However, this benefit was counterbalanced by a significant delay in platelet engraftment (21 versus 17 d, < 0.001). Multivariate logistic regression analysis identified mismatched donors (odds ratio, 1.72; 95% confidence interval, 1.03-2.88; = 0.038) and the duration of G-CSF therapy (odds ratio, 1.04; 95% confidence interval, 1.00-1.09; = 0.038) as independent predictors for the development of ES. Despite these hematological impacts, there was no observed advantage in overall survival, nonrelapse mortality, or graft-versus-host disease-free/relapse-free survival among patients who received G-CSF compared with those who did not.
Although G-CSF post-HCT expedited neutrophil engraftment and reduced BSI risk, it did not result in a survival advantage. The association with ES necessitates careful consideration.
尽管异基因造血细胞移植(HCT)后生长因子已应用数十年,但其作用仍不明确,引发了持续的争论和研究。生长因子的理论影响在众多研究中受到了挑战。
在玛格丽特公主癌症中心进行的这项回顾性队列研究中,我们分析了2019年5月1日至2022年5月31日期间接受异基因HCT的509例患者的临床结局。本研究旨在评估移植后给予粒细胞集落刺激因子(G-CSF)对中性粒细胞和血小板植入、血流感染(BSI)发生率、移植物抗宿主病、植入综合征(ES)以及生存指标(包括总生存、非复发死亡率和无移植物抗宿主病/无复发生存)的影响。
我们的研究结果表明,给予G-CSF可加速中性粒细胞植入(16天对18天,P = 0.009),并与BSI发生率降低相关(9.4%对31.3%,P = 0.014)。然而,这一益处被血小板植入显著延迟所抵消(21天对17天,P < 0.001)。多因素逻辑回归分析确定,供者不匹配(比值比,1.72;95%置信区间,1.03 - 2.88;P = 0.038)和G-CSF治疗持续时间(比值比,1.04;95%置信区间,1.00 - 1.09;P = 0.038)是ES发生的独立预测因素。尽管有这些血液学影响,但与未接受G-CSF的患者相比,接受G-CSF的患者在总生存、非复发死亡率或无移植物抗宿主病/无复发生存方面未观察到优势。
尽管HCT后给予G-CSF可加速中性粒细胞植入并降低BSI风险,但并未带来生存优势。与ES的关联需要仔细考虑。