Soussi Sabri, Tarvasmäki Tuukka, Kimmoun Antoine, Ahmadiankalati Mojtaba, Azibani Feriel, Dos Santos Claudia C, Duarte Kevin, Gayat Etienne, Jentzer Jacob C, Harjola Veli-Pekka, Hibbert Benjamin, Jung Christian, Johan Lassus, Levy Bruno, Lu Zihang, Lawler Patrick R, Marshall John C, Pöss Janine, Sadoune Malha, Nguyen Alexis, Raynor Alexandre, Peoc'h Katell, Thiele Holger, Mathew Rebecca, Mebazaa Alexandre
Department of Anesthesiology and Pain Medicine, University of Toronto, Toronto, Ontario, Canada.
University of Paris Cité, Inserm UMR-S 942, Cardiovascular Markers in Stress Conditions (MASCOT), Paris, France.
EClinicalMedicine. 2024 Dec 18;79:103013. doi: 10.1016/j.eclinm.2024.103013. eCollection 2025 Jan.
Cardiogenic shock (CS) is a heterogeneous clinical syndrome, making it challenging to predict patient trajectory and response to treatment. This study aims to identify biological/molecular CS subphenotypes, evaluate their association with outcome, and explore their impact on heterogeneity of treatment effect (ShockCO-OP, NCT06376318).
We used unsupervised clustering to integrate plasma biomarker data from two prospective cohorts of CS patients: CardShock (N = 205 [2010-2012, NCT01374867]) and the French and European Outcome reGistry in Intensive Care Units (FROG-ICU) (N = 228 [2011-2013, NCT01367093]) to determine the optimal number of classes. Thereafter, a simplified classifier (Euclidean distances) was used to assign the identified CS subphenotypes in three completed randomized controlled trials (RCTs) (OptimaCC, N = 57 [2011-2016, NCT01367743]; DOREMI, N = 192 [2017-2020, NCT03207165]; and CULPRIT-SHOCK, N = 434 [2013-2017, NCT01927549]) and explore heterogeneity of treatment effect with respect to 28-day mortality (primary outcome).
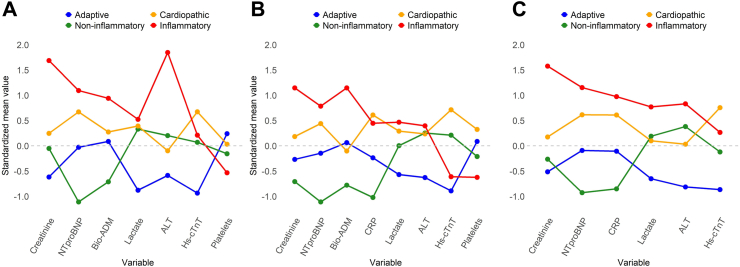
Four biomarker-driven CS subphenotypes ('adaptive', 'non-inflammatory', 'cardiopathic', and 'inflammatory') were identified separately in the two cohorts. Patients in the inflammatory and cardiopathic subphenotypes had the highest 28-day mortality (p (log-rank test) = 0.0099 and 0.0055 in the CardShock and FROG-ICU cohorts, respectively). Subphenotype membership significantly improved risk stratification when added to traditional risk factors including the Society for Cardiovascular Angiography and Interventions (SCAI) shock stages (increase in Harrell's C-index by 4% ( = 0.033) and 6% ( = 0.0068) respectively in the CardShock and the FROG-ICU cohorts). The simplified classifier identified CS subphenotypes with similar biological/molecular and outcome characteristics in the three independent RCTs. No significant interaction was observed between treatment effect and subphenotypes.
Subphenotypes with the highest concentration of biomarkers of endothelial dysfunction and inflammation (inflammatory) or myocardial injury/fibrosis (cardiopathic) were associated with mortality independently from the SCAI shock stages.
Dr Sabri Soussi was awarded the Canadian Institutes of Health Research (CIHR) Doctoral Foreign Study Award (DFSA) and the Merit Awards Program (Department of Anesthesiology and Pain Medicine, University of Toronto, Canada) for the current study.
心源性休克(CS)是一种异质性临床综合征,这使得预测患者病程及对治疗的反应具有挑战性。本研究旨在识别生物学/分子层面的心源性休克亚表型,评估其与预后的关联,并探讨其对治疗效果异质性的影响(休克合作研究,NCT06376318)。
我们采用无监督聚类方法,整合来自两个心源性休克患者前瞻性队列的数据:心脏休克队列(N = 205 [2010 - 2012年,NCT01374867])以及法国和欧洲重症监护病房结局注册研究(FROG - ICU)(N = 228 [2011 - 2013年,NCT01367093]),以确定最佳类别数量。此后,使用一种简化分类器(欧几里得距离)在三项完成的随机对照试验(RCT)中分配已识别的心源性休克亚表型(最佳心脏骤停后治疗,N = 57 [2011 - 2016年,NCT01367743];多模式心肺复苏与靶向温度管理试验,N = 192 [2017 - 2020年,NCT03207165];以及心源性休克罪犯血管血运重建术与最佳药物治疗试验,N = 434 [2013 - 2017年,NCT01927549]),并探讨28天死亡率(主要结局)方面的治疗效果异质性。
在两个队列中分别识别出四种由生物标志物驱动的心源性休克亚表型(“适应性”、“非炎症性”、“心源性”和“炎症性”)。炎症性和心源性亚表型的患者28天死亡率最高(心脏休克队列中p(对数秩检验)= 0.0099,FROG - ICU队列中p = 0.0055)。当将亚表型归属添加到包括心血管造影和介入学会(SCAI)休克分期在内的传统危险因素中时,显著改善了风险分层(心脏休克队列和FROG - ICU队列中Harrell氏C指数分别增加4%(p = 0.033)和6%(p = 0.0068))。简化分类器在三项独立的随机对照试验中识别出具有相似生物学/分子及结局特征的心源性休克亚表型。未观察到治疗效果与亚表型之间存在显著相互作用。
内皮功能障碍和炎症生物标志物浓度最高的亚表型(炎症性)或心肌损伤/纤维化亚表型(心源性)与死亡率相关,独立于SCAI休克分期。
Sabri Soussi博士获得了加拿大卫生研究院(CIHR)博士国外研究奖(DFSA)以及(加拿大多伦多大学麻醉学与疼痛医学系)卓越奖计划,用于当前研究。