Catarci Stefano, Zanfini Bruno Antonio, Scorzoni Marco, De Martino Salvatore, Giuri Pietro Paolo, Frassanito Luciano, Gonnella Gian Luigi, Capone Emanuele, Di Maio Francesco Vitale, Maddaloni Giovanni, Lanzone Antonio, Draisci Gaetano
Department of Scienze Dell'Emergenza, Anestesiologiche e Della Rianimazione, IRCCS Fondazione Policlinico A. Gemelli, Rome, Italy.
Department of Scienze della Salute della Donna, del Bambino e di Sanità Pubblica, IRCCS Fondazione Policlinico A. Gemelli, Rome, Italy.
BMC Anesthesiol. 2025 Jan 20;25(1):32. doi: 10.1186/s12871-024-02871-5.
Improvements in diagnostics and clinical care have allowed more women of childbearing age, suffering from neurological diseases, to safely have pregnancy, reducing peripartum complications. However, these patients remain at risk and are a constant challenge for anesthesiologists in the delivery room.
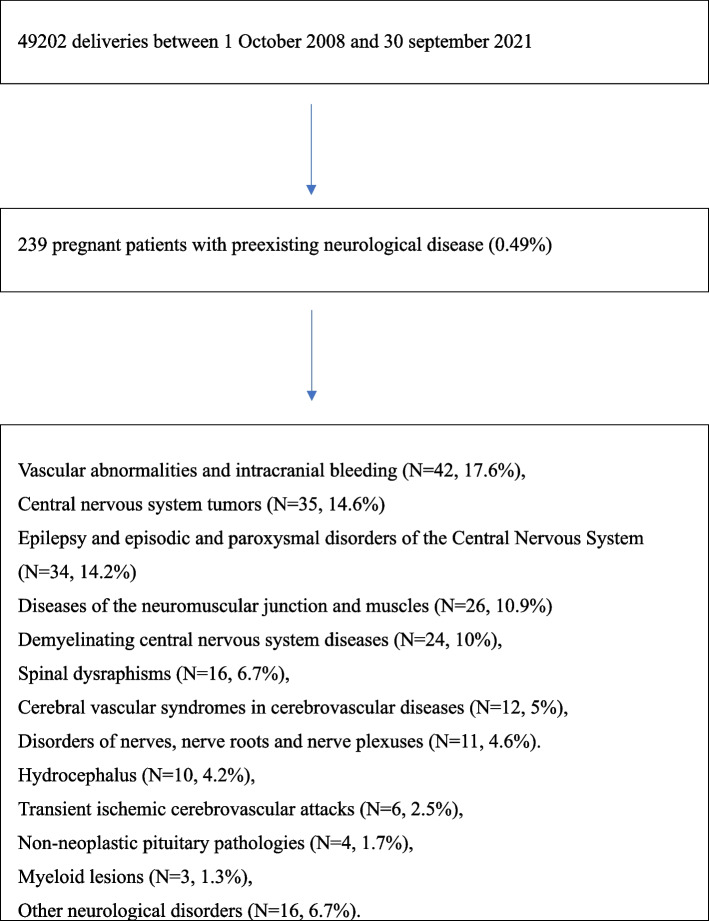
To assess the type of anesthesiologic management performed for delivery in obstetric patients with preexisting neurological disease and who reported significant neurological symptoms during pregnancy, a retrospective observational study was carried out between 1 October 2008 and 30 September 2021.
Data from 49,202 pregnant women were assessed over 13 years; 239 pregnant women with a diagnosis of preexisting neurological disease and who reported significant neurological symptoms during pregnancy were identified (prevalence 0.49%). The main neurological disorders that affected pregnant women included vascular abnormalities and intracranial bleeding (N = 42, 17.6%), central nervous system tumors (N = 35, 14.6%), epilepsy and episodic and paroxysmal disorders of the central nervous system (N = 34, 14.2%), diseases of the neuromuscular junction and muscles (N = 26, 10.9%), demyelinating central nervous system diseases (N = 24, 10%). A total of 234 (97.9%) pregnant women with neurological disorders and significant neurological symptoms underwent cesarean section: 192 (80.3% of the total cesarean sections) were elective, 39 (16.3%) were urgent type 2 and 3; 3 (1.2%) were emergency cesarean sections. General anesthesia was administered to 73 patients (30.5%), while 166 patients (69.5%) were managed with neuraxial techniques. 2 patients who had had neuraxial block reported worsening neurological symptoms that required a change in medical therapy. Postoperative multiparameter monitoring was performed for less than 24 h in the recovery room for 226 patients (94.6%). 3 patients (1.2%) were observed with multiparameter monitoring in the post-anesthesia care unit (PACU) for more than 24 hours; 10 patients (4.2%) were moved to the postoperative intensive care unit (ICU). The median hospitalization duration was 4 days (with an interquartile difference of 3-6 days).
In our experience, when neuraxial anesthesia was feasible, it proved to be a safe option for pregnant patients with symptomatic neurological disease, resulting in uncommon maternal complications.
诊断和临床护理的改善使更多患有神经系统疾病的育龄妇女能够安全怀孕,减少围产期并发症。然而,这些患者仍面临风险,对产房的麻醉医生来说始终是一项挑战。
为评估对患有神经系统疾病且在孕期出现明显神经症状的产科患者进行分娩时的麻醉管理类型,于2008年10月1日至2021年9月30日开展了一项回顾性观察研究。
在13年期间评估了49202名孕妇的数据;确定了239名诊断为患有神经系统疾病且在孕期出现明显神经症状的孕妇(患病率0.49%)。影响孕妇的主要神经系统疾病包括血管异常和颅内出血(42例,17.6%)、中枢神经系统肿瘤(35例,14.6%)、癫痫及中枢神经系统发作性和阵发性疾病(34例,14.2%)、神经肌肉接头和肌肉疾病(26例,10.9%)、中枢神经系统脱髓鞘疾病(24例,10%)。共有234名(97.9%)患有神经系统疾病且有明显神经症状的孕妇接受了剖宫产:192例(占剖宫产总数的80.3%)为择期剖宫产,39例(16.3%)为2级和3级紧急剖宫产;3例(1.2%)为急诊剖宫产。73例患者(30.5%)接受了全身麻醉,而166例患者(69.5%)采用了神经轴技术管理。2例接受神经轴阻滞的患者报告神经症状恶化,需要改变治疗方案。226例患者(94.6%)在恢复室进行了不到24小时的术后多参数监测。3例患者(1.2%)在麻醉后护理单元(PACU)接受了超过24小时的多参数监测;10例患者(4.2%)被转移到术后重症监护病房(ICU)。中位住院时间为4天(四分位间距为3 - 6天)。
根据我们的经验,当可行时,神经轴麻醉对有症状的神经系统疾病孕妇来说是一种安全的选择,产妇并发症不常见。