Mohan Viswanathan
Madras Diabetes Research Foundation and Dr. Mohan's Diabetes Specialities Centre, Chennai, India.
Diabetes Care. 2025 Feb 1;48(2):153-163. doi: 10.2337/dci24-0046.
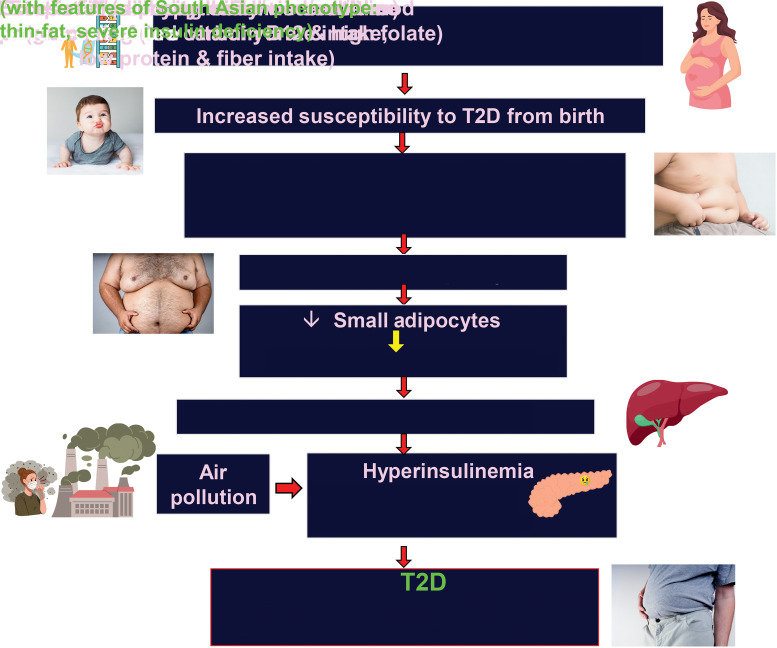
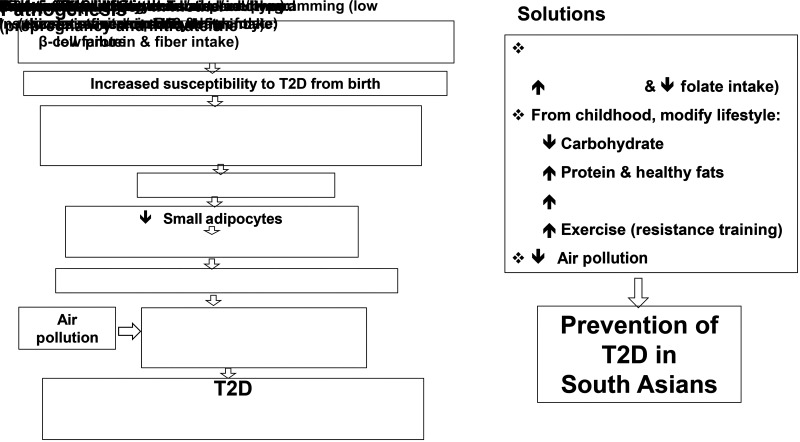
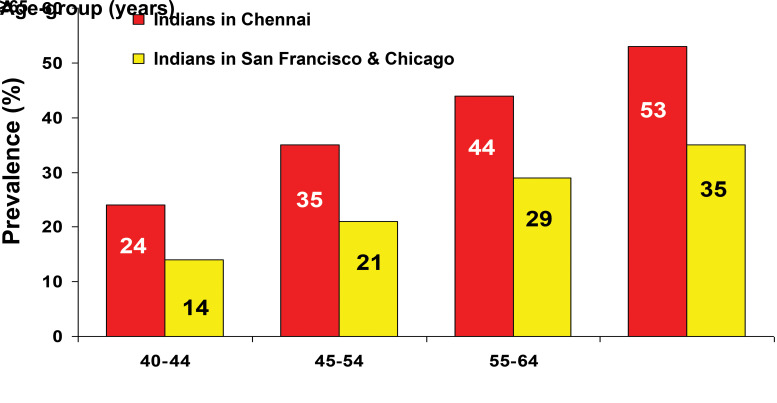
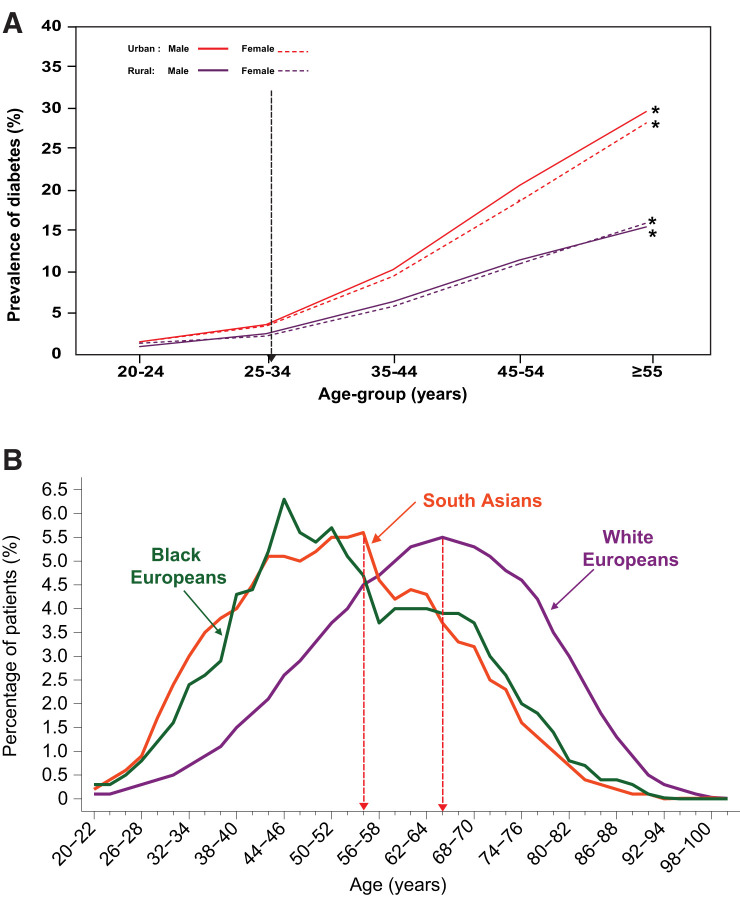
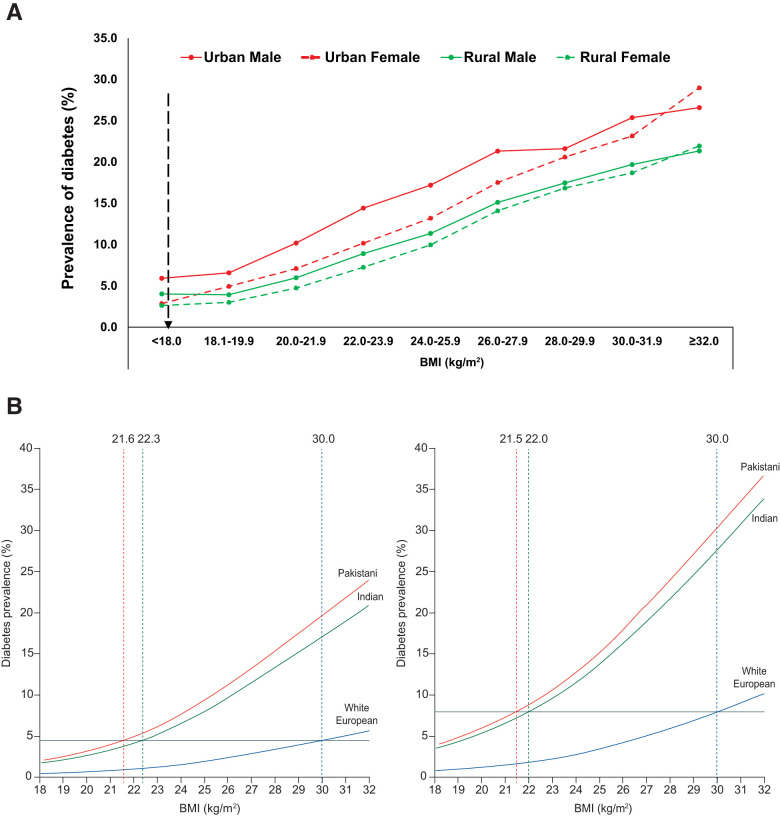
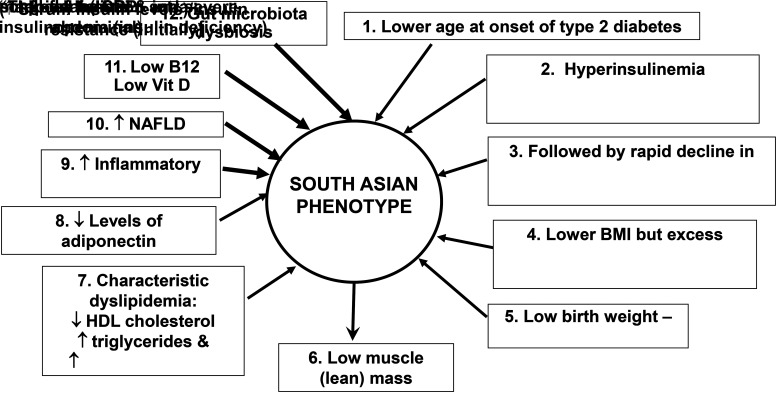
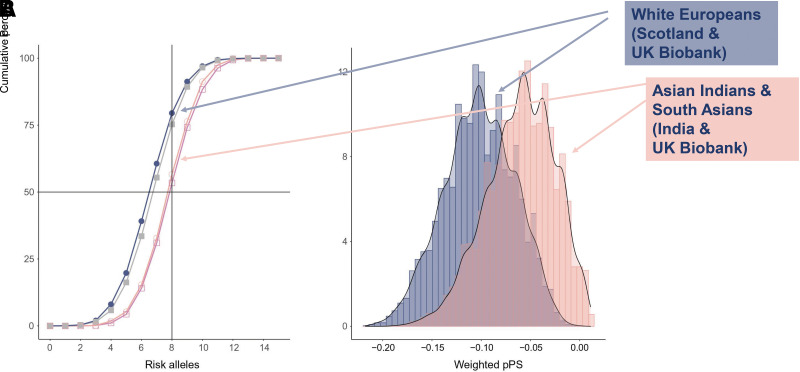
South Asia has high prevalence rates of type 2 diabetes (T2D). Until the 1990s, the prevalence of T2D within South Asia was low but much higher in the South Asian diaspora living abroad. Today, high prevalence rates of T2D are reported among those living in South Asia. T2D in South Asians presents with unique clinical features described as the "South Asian phenotype" that include younger age at onset of diabetes than in White Europeans, much lower BMI, hyperinsulinemia and greater insulin resistance, rapid decline in β-cell function resulting in low insulin reserve, low muscle mass, and greater ectopic fat deposition, especially in the liver. Also, prevalence of impaired fasting glucose is higher among South Asians than prevalence of impaired glucose tolerance. Genetic predisposition combined with intrauterine fetal programming (low vitamin B12 intake and high folate intake) increases susceptibility to T2D, from birth. In later life, overnutrition, especially a high carbohydrate intake with refined grains of higher glycemic index, coupled with low physical activity likely triggers the T2D epidemic in South Asians. Additionally, there are emerging risk factors like air pollution. Preventing T2D in South Asians requires a multifactorial approach, including improvements in maternal and fetal nutrition with special reference to vitamin B12 and folate intake, decreasing refined carbohydrate and increasing protein and fiber intake in the diet, increasing physical activity, and control of air pollution. Lessons learned from epidemiology of T2D in South Asians could be useful to other developing countries that are in earlier stages of epidemiological transition.
南亚2型糖尿病(T2D)的患病率很高。直到20世纪90年代,南亚地区T2D的患病率较低,但在海外生活的南亚侨民中患病率要高得多。如今,据报道生活在南亚的人群中T2D患病率很高。南亚人的T2D具有独特的临床特征,被称为“南亚表型”,包括糖尿病发病年龄比欧洲白人更年轻、体重指数(BMI)低得多、高胰岛素血症和更高的胰岛素抵抗、β细胞功能迅速下降导致胰岛素储备低、肌肉量低以及异位脂肪沉积更多,尤其是在肝脏。此外,南亚人空腹血糖受损的患病率高于糖耐量受损的患病率。遗传易感性与子宫内胎儿编程(维生素B12摄入量低和叶酸摄入量高)相结合,从出生起就增加了患T2D的易感性。在晚年,营养过剩,尤其是高碳水化合物摄入量以及高血糖指数的精制谷物,再加上低体力活动,可能引发南亚人的T2D流行。此外,还有空气污染等新出现的危险因素。预防南亚人的T2D需要采取多因素方法,包括改善孕产妇和胎儿营养,特别关注维生素B12和叶酸摄入量,减少饮食中精制碳水化合物的摄入并增加蛋白质和纤维摄入量,增加体力活动,以及控制空气污染。从南亚人T2D流行病学中吸取的经验教训可能对处于流行病学转变早期阶段的其他发展中国家有用。