Gopalan Narendran, Viswanathan Vinod Kumar, Srinivasalu Vignes Anand, Arumugam Saranya, Bhaskar Adhin, Manoharan Tamizhselvan, Chandrasekar Santosh Kishor, Bujagaruban Divya, Arumugham Ramya, Jagadeeswaran Gopi, Pandian Saravanan Madurai, Ponniah Arunalatha, Senguttuvan Thirumaran, Chinnaiyan Ponnuraja, Dhanraj Baskaran, Chadha Vineet Kumar, Purushotham Balaji, Murhekar Manoj Vasanth
ICMR-NIRT-Indian Council of Medical Research -National Institute for Research in Tuberculosis, Chetpet, Chennai, India.
GSMC-Government Stanley Medical College and Hospital, Chennai, India.
PLoS One. 2025 Jan 24;20(1):e0312993. doi: 10.1371/journal.pone.0312993. eCollection 2025.
Judicious utilisation of tertiary care facilities through appropriate risk stratification assumes priority, in a raging pandemic, of the nature of delta variant-predominated second wave of COVID-19 pandemic in India. Prioritisation of tertiary care, through a scientifically validated risk score, would maximise recovery without compromising individual safety, but importantly without straining the health system.
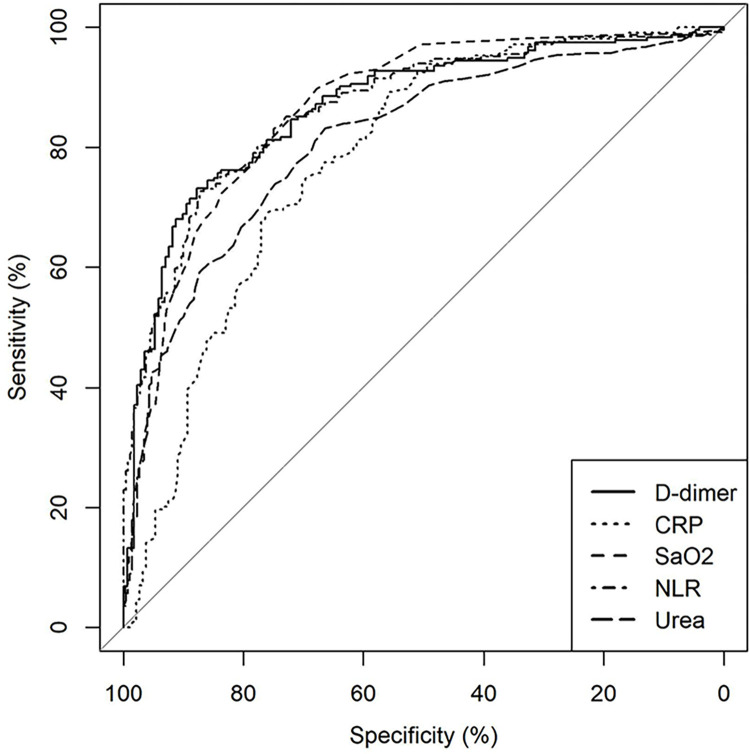
De-identified data of COVID-19 confirmed patients admitted to a tertiary care hospital in South India, between April 1, 2021 and July 31, 2021, corresponding to the peak of COVID-19 second wave, were analysed after segregating into 'survivors' or 'non-survivors' to evaluate the risk factors for COVID-19 mortality at admission and formulate a risk score with easily obtainable but clinically relevant parameters for accurate patient triaging. The predictive ability was ascertained by the area under the receiver operator characteristics (AUROC) and the goodness of fit by the Hosmer-Lemeshow test and validated using the bootstrap method.
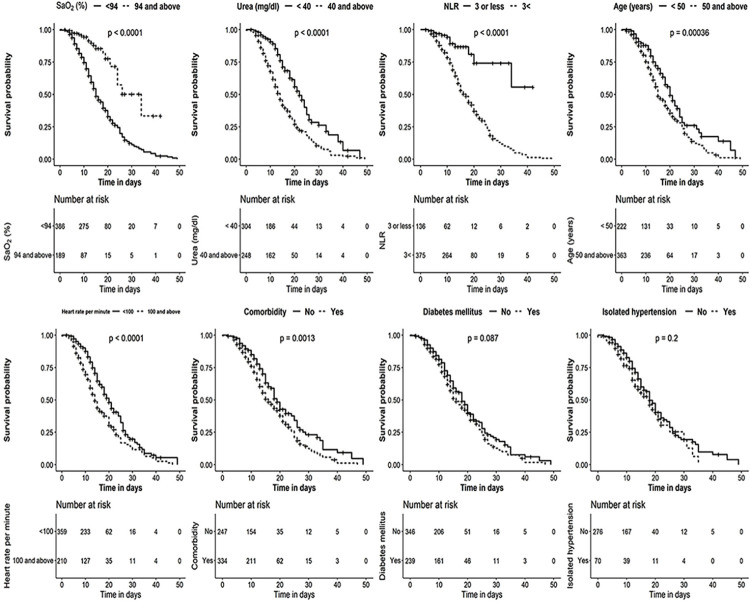
Of 617 COVID-19 patients (325 survivors, 292 non-survivors), treated as per prevailing national guidelines, with a slight male predilection (358/617 [58.0%]), fatalities in the age group above and below 50 years were (217/380 [57.1%]) and (75/237 [31.6%]), p<0.001. The relative distribution of the various parameters among survivors and non-survivors including self-reported comorbidities helped to derive the individual risk scores from parameters significant in the multivariable logistic regression. The 'OUR-ARCad' risk score components were-Oxygen saturation SaO2<94%-23, Urea > 40mg/dL-15, Neutrophil/Lymphocytic ratio >3-23, Age > 50 years-8, Pulse Rate >100-8 and Coronary Artery disease-15. A summated score above 50, mandated tertiary care management (sensitivity-90%, specificity-75%; AUC-0.89), validated in 2000 bootstrap dataset.
The OUR-ARCad risk score, could potentially maximize recovery in a raging COVID-19 pandemic, through prioritisation of tertiary care services, neither straining the health system nor compromising patient's safety, delivering and diverting care to those who needed the most.
在印度由德尔塔变异株主导的第二波新冠疫情肆虐期间,通过适当的风险分层明智地利用三级医疗设施成为当务之急。通过科学验证的风险评分对三级医疗进行优先排序,将在不影响个人安全的情况下最大限度地提高康复率,而且重要的是不会给卫生系统造成压力。
对2021年4月1日至2021年7月31日期间入住印度南部一家三级医院的新冠确诊患者的去识别化数据进行分析,这段时间对应新冠疫情第二波高峰期。将患者分为“幸存者”或“非幸存者”,以评估入院时新冠死亡的风险因素,并使用易于获取但具有临床相关性的参数制定风险评分,用于准确的患者分流。通过受试者操作特征曲线下面积(AUROC)确定预测能力,通过Hosmer-Lemeshow检验确定拟合优度,并使用自助法进行验证。
在按照现行国家指南治疗的617例新冠患者中(325例幸存者,292例非幸存者),男性略多(358/617 [58.0%]),50岁及以上和50岁以下年龄组的死亡人数分别为(217/380 [57.1%])和(75/237 [31.6%]),p<0.001。包括自我报告的合并症在内的幸存者和非幸存者之间各种参数的相对分布有助于从多变量逻辑回归中具有显著意义的参数得出个体风险评分。“OUR-ARCad”风险评分的组成部分为:血氧饱和度SaO2<94%-23分、尿素>40mg/dL-15分、中性粒细胞/淋巴细胞比值>3-23分、年龄>50岁-8分、脉搏率>100-8分和冠状动脉疾病-15分。总分超过50分需要三级医疗管理(敏感性-90%,特异性-75%;AUC-0.89),在2000个自助数据集中得到验证。
“OUR-ARCad”风险评分有可能在肆虐的新冠疫情中通过优先安排三级医疗服务,既不给卫生系统造成压力,也不危及患者安全,将护理提供给最需要的人并实现分流,从而最大限度地提高康复率。