Department of Clinical Research, ICMR-National Institute for Research in Tuberculosis (Formerly Tuberculosis Research Centre), Chennai, Tamil Nadu, India.
Department of General Medicine, Government Chengalpattu Medical College & Hospital, Chengalpattu, Tamil Nadu, India.
PLoS One. 2022 Feb 3;17(2):e0263471. doi: 10.1371/journal.pone.0263471. eCollection 2022.
We retrospectively data-mined the case records of Reverse Transcription Polymerase Chain Reaction (RT-PCR) confirmed COVID-19 patients hospitalized to a tertiary care centre to derive mortality predictors and formulate a risk score, for prioritizing admission.
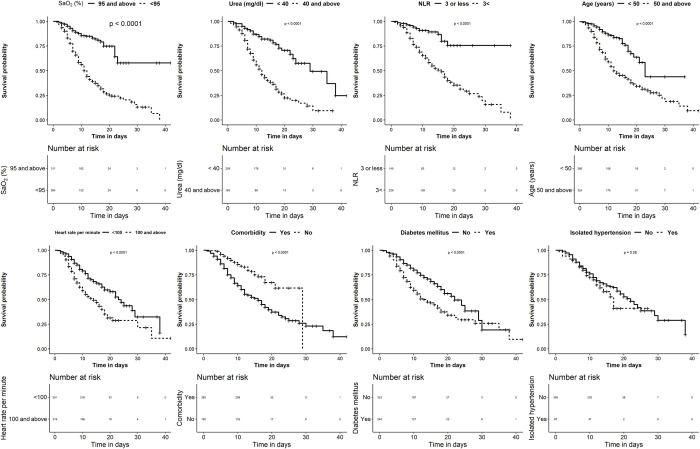
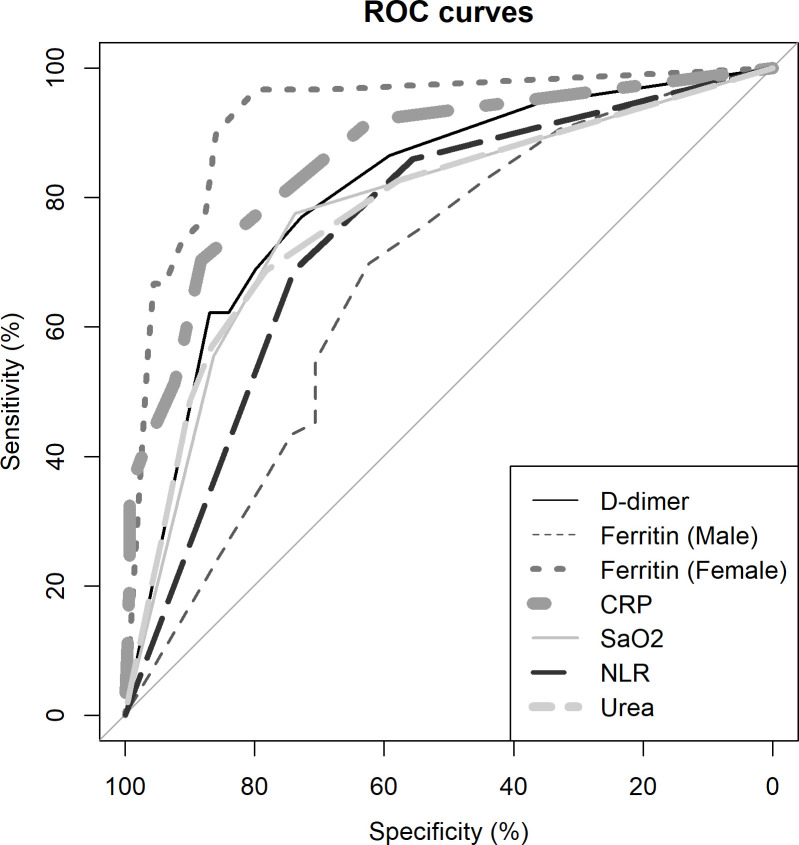
Data on clinical manifestations, comorbidities, vital signs, and basic lab investigations collected as part of routine medical management at admission to a COVID-19 tertiary care centre in Chengalpattu, South India between May and November 2020 were retrospectively analysed to ascertain predictors of mortality in the univariate analysis using their relative difference in distribution among 'survivors' and 'non-survivors'. The regression coefficients of those factors remaining significant in the multivariable logistic regression were utilised for risk score formulation and validated in 1000 bootstrap datasets. Among 746 COVID-19 patients hospitalised [487 "survivors" and 259 "non-survivors" (deaths)], there was a slight male predilection [62.5%, (466/746)], with a higher mortality rate observed among 40-70 years age group [59.1%, (441/746)] and highest among diabetic patients with elevated urea levels [65.4% (68/104)]. The adjusted odds ratios of factors [OR (95% CI)] significant in the multivariable logistic regression were SaO2<95%; 2.96 (1.71-5.18), Urea ≥50 mg/dl: 4.51 (2.59-7.97), Neutrophil-lymphocytic ratio (NLR) >3; 3.01 (1.61-5.83), Age ≥50 years;2.52 (1.45-4.43), Pulse Rate ≥100/min: 2.02 (1.19-3.47) and coexisting Diabetes Mellitus; 1.73 (1.02-2.95) with hypertension and gender not retaining their significance. The individual risk scores for SaO2<95-11, Urea ≥50 mg/dl-15, NLR >3-11, Age ≥50 years-9, Pulse Rate ≥100/min-7 and coexisting diabetes mellitus-6, acronymed collectively as 'OUR-ARDs score' showed that the sum of scores ≥ 25 predicted mortality with a sensitivity-90%, specificity-64% and AUC of 0.85.
The 'OUR ARDs' risk score, derived from easily assessable factors predicting mortality, offered a tangible solution for prioritizing admission to COVID-19 tertiary care centre, that enhanced patient care but without unduly straining the health system.
我们回顾性地挖掘了经逆转录聚合酶链反应(RT-PCR)确诊的 COVID-19 住院患者的病历记录,以确定死亡率预测因素并制定风险评分,以便优先入院。
在印度南部 Chengalpattu 的一家 COVID-19 三级护理中心,我们对 2020 年 5 月至 11 月期间入院时常规医疗管理中收集的临床表现、合并症、生命体征和基本实验室检查数据进行了回顾性分析,以确定单变量分析中死亡率的预测因素,方法是使用幸存者和非幸存者之间分布的相对差异。在多变量逻辑回归中仍然具有统计学意义的这些因素的回归系数用于风险评分的制定,并在 1000 个 bootstrap 数据集中进行验证。在 746 名 COVID-19 住院患者中[487 名“幸存者”和 259 名“非幸存者”(死亡)],男性略占优势[62.5%(466/746)],40-70 岁年龄组死亡率较高[59.1%(441/746)],最高的是尿素水平升高的糖尿病患者[65.4%(68/104)]。多变量逻辑回归中具有统计学意义的因素[比值比(95%CI)]的调整后比值 SaO2<95%;2.96(1.71-5.18),尿素≥50mg/dl:4.51(2.59-7.97),中性粒细胞-淋巴细胞比值(NLR)>3;3.01(1.61-5.83),年龄≥50 岁;2.52(1.45-4.43),脉搏率≥100/min:2.02(1.19-3.47)和并存的糖尿病;1.73(1.02-2.95),高血压和性别不再具有统计学意义。SaO2<95-11、Urea≥50mg/dl-15、NLR>3-11、Age≥50 岁-9、Pulse Rate≥100/min-7 和并存糖尿病的个体风险评分分别为 6,统称为“OUR-ARDs 评分”,结果表明,评分总和≥25 可预测死亡率,其敏感性为 90%,特异性为 64%,AUC 为 0.85。
从可评估的死亡率预测因素中得出的“OUR ARDs”风险评分,为 COVID-19 三级护理中心的入院提供了一个切实可行的解决方案,增强了患者护理,但并未给卫生系统带来过度压力。