State Key Laboratory of Cardiovascular Disease, Beijing, China.
Cardiometabolic Medicine Center, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, 167A Beilishi Road, Xi Cheng District, Beijing, 100037, China.
Cardiovasc Diabetol. 2022 Aug 13;21(1):156. doi: 10.1186/s12933-022-01583-9.
Inflammation plays a crucial role in the pathogenesis and progression of coronary artery disease (CAD). The neutrophil to lymphocyte ratio (NLR) is a novel inflammatory biomarker and its association with clinical outcomes in CAD patients with different glycemic metabolism after percutaneous coronary intervention (PCI) remains undetermined. Therefore, this study aimed to investigate the effect of NLR on the prognosis of patients undergoing PCI with or without type 2 diabetes mellitus (T2DM).
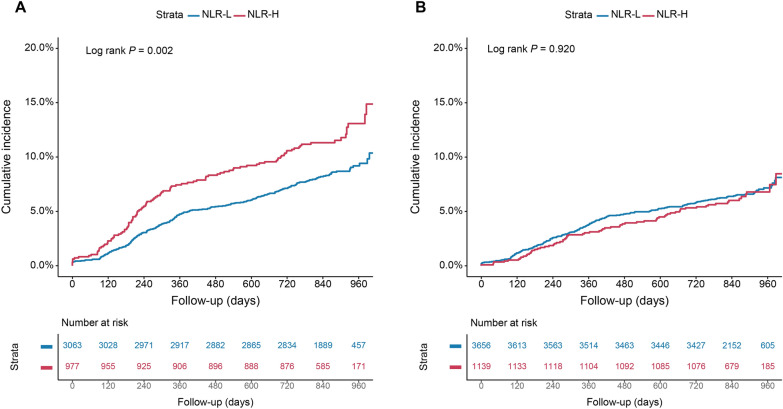
We consecutively enrolled 8,835 patients with CAD hospitalized for PCI at Fuwai hospital. NLR was calculated using the following formula: neutrophil (*10/L)/lymphocyte (*10/L). According to optimal cut-off value, study patients were categorized as higher level of NLR (NLR-H) and lower level of NLR (NLR-L) and were further stratified as NLR-H with T2DM and non-T2DM, and NLR-L with T2DM and non-T2DM. The primary endpoint was major adverse cardiovascular and cerebrovascular events (MACCEs), defined as all-cause mortality, myocardial infarction (MI), stroke and target vessel revascularization.
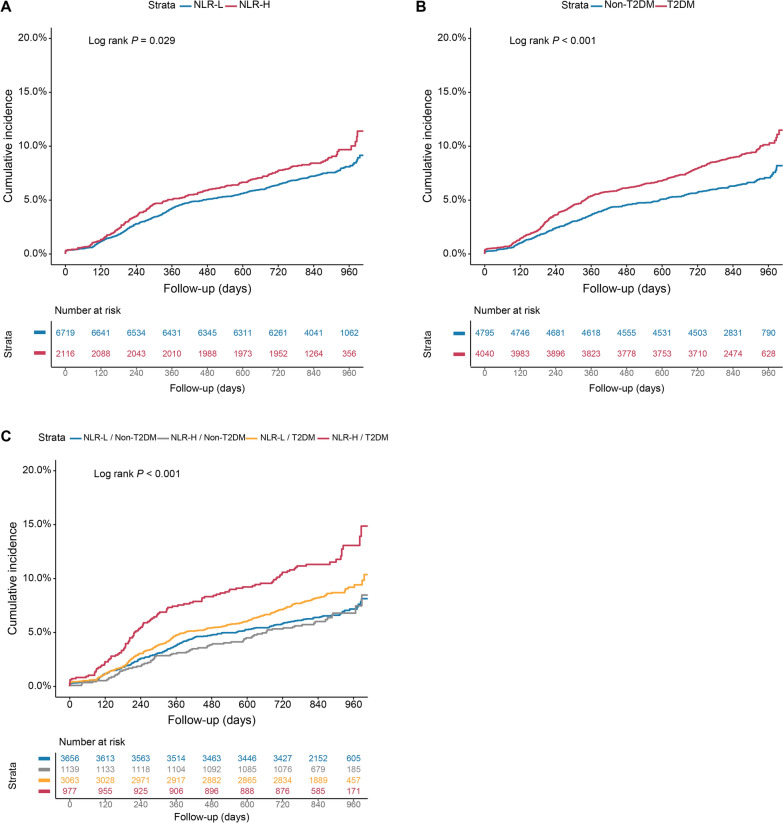
A total of 674 (7.6%) MACCEs were recorded during a median follow-up of 2.4 years. The optimal cut-off value of NLR was 2.85 determined by the surv_cutpoint function. Compared to those in the NLR-H/T2DM groups, patients in the NLR-L/non-T2DM, NLR-H/non-T2DM and NLR-L/T2DM groups were at significantly lower risk of 2-year MACCEs [adjusted hazard ratio (HR): 0.67, 95% confidence interval (CI): 0.52 to 0.87, P = 0.003; adjusted HR: 0.62, 95%CI: 0.45 to 0.85, P = 0.003; adjusted HR: 0.77, 95%CI: 0.61 to 0.97, P = 0.025; respectively]. Remarkably, patients in the NLR-L/non-T2DM group also had significantly lower risk of a composite of all-cause mortality and MI than those in the NLR-H/T2DM group (adjusted HR: 0.57, 95%CI: 0.35 to 0.93, P = 0.024). Multivariable Cox proportional hazards model also indicated the highest risk of MACCEs in diabetic patients with higher level of NLR than others (P for trend = 0.009). Additionally, subgroup analysis indicated consistent impact of NLR on MACCEs across different subgroups.
Presence of T2DM with elevated NLR is associated with worse clinical outcomes in CAD patients undergoing PCI. Categorization of patients with elevated NLR and T2DM could provide valuable information for risk stratification of CAD patients.
炎症在冠状动脉疾病(CAD)的发病机制和进展中起着关键作用。中性粒细胞与淋巴细胞比值(NLR)是一种新的炎症生物标志物,但其与经皮冠状动脉介入治疗(PCI)后不同血糖代谢 CAD 患者的临床结局之间的关系尚不确定。因此,本研究旨在探讨 NLR 对接受或不接受 2 型糖尿病(T2DM)PCI 的患者预后的影响。
我们连续纳入了在阜外医院因 CAD 住院接受 PCI 的 8835 例患者。NLR 通过以下公式计算:中性粒细胞(*10/L)/淋巴细胞(*10/L)。根据最佳截断值,研究患者分为 NLR 较高组(NLR-H)和 NLR 较低组(NLR-L),并进一步分为 NLR-H 伴 T2DM 和非 T2DM 组,以及 NLR-L 伴 T2DM 和非 T2DM 组。主要心血管不良事件(MACCEs)为主要终点,定义为全因死亡率、心肌梗死(MI)、卒中和靶血管血运重建。
在中位数为 2.4 年的随访期间,共记录了 674 例(7.6%)MACCEs。通过 surv_cutpoint 函数确定 NLR 的最佳截断值为 2.85。与 NLR-H/T2DM 组相比,NLR-L/非 T2DM、NLR-H/非 T2DM 和 NLR-L/T2DM 组患者 2 年 MACCEs 的风险显著降低[校正风险比(HR):0.67,95%置信区间(CI):0.52 至 0.87,P=0.003;校正 HR:0.62,95%CI:0.45 至 0.85,P=0.003;校正 HR:0.77,95%CI:0.61 至 0.97,P=0.025;分别]。值得注意的是,与 NLR-H/T2DM 组相比,NLR-L/非 T2DM 组患者全因死亡率和 MI 的复合终点风险也显著降低(校正 HR:0.57,95%CI:0.35 至 0.93,P=0.024)。多变量 Cox 比例风险模型还表明,与其他组相比,伴升高 NLR 的糖尿病患者发生 MACCEs 的风险最高(P 趋势=0.009)。此外,亚组分析表明,NLR 对 MACCEs 的影响在不同亚组中一致。
在接受 PCI 的 CAD 患者中,T2DM 伴 NLR 升高与更差的临床结局相关。伴升高 NLR 和 T2DM 的患者分类可为 CAD 患者的风险分层提供有价值的信息。