Kitagawa Daiki, Uedo Noriya, Hanaoka Noboru, Kanesaka Takashi, Tani Yasuhiro, Okubo Yuki, Asada Yuya, Ueda Tomoya, Kizawa Atsuko, Ninomiya Takehiro, Ando Yoshiaki, Tanabe Gentaro, Fujimoto Yuta, Hitoshi Mori, Kato Minoru, Yoshii Shunsuke, Shichijo Satoki, Yamamoto Sachiko, Higashino Koji, Michida Tomoki, Ishihara Ryu, Fujiwara Yasuhiro
Gastrointestinal Oncology, Osaka International Cancer Institute, Osaka, Japan.
Gastroenterology, Osaka Metropolitan University Graduate School of Medicine School of Medicine, Osaka, Japan.
Endosc Int Open. 2025 Jan 29;13:a24517835. doi: 10.1055/a-2451-7835. eCollection 2025.
Emergency surgery is usually required for patients with delayed perforation after gastric endoscopic submucosal dissection (ESD); however, cases of successful endoscopic treatment recently have been reported. Here, we elucidated the usefulness of endoscopic intervention for patients with delayed perforation.
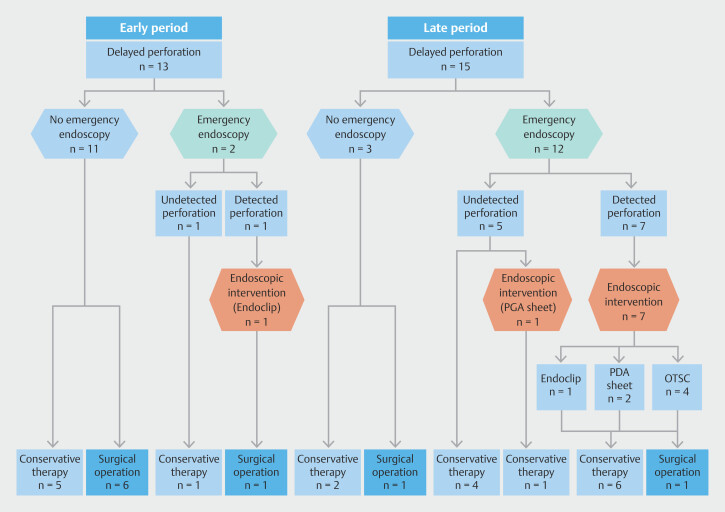
Patients who underwent gastric ESD from 2005 to 2022 were assessed for eligibility. Delayed perforation was defined as no intraprocedural perforation after the ESD but subsequent development of peritoneal irritation and free air on computed tomography scan. Participants were divided into early- and late-period groups based on time (October 2015) of implementation of the polyglycolic acid (PGA) sheet and the over-the-scope clip (OTSC) in clinical practice. We evaluated changes in incidence of required surgery.
Among the 5,048 patients who underwent gastric ESD, delayed perforation occurred in 28 patients (0.6%, 95% confidence interval [CI] 0.4%-0.8%). Incidence of delayed perforation did not differ significantly between the early- and late-period groups (0.5% vs. 0.6%). The proportion of patients who underwent surgery was significantly smaller in the late-period group than in the early-period group (54% vs. 13%, odds ratio [OR] 0.14, 95% CI 0.02-0.83; = 0.042); this was confirmed by multivariate analysis (adjusted OR 0.04, 95% CI 0.002-0.9; = 0.043) after adjustment for age, sex, Charlson's comorbidity index, tumor location, and size.
Endoscopic intervention using PGA sheets and OTSC was associated with a low incidence of required surgery for delayed perforation after gastric ESD and is recommended.
胃内镜黏膜下剥离术(ESD)后发生延迟穿孔的患者通常需要急诊手术;然而,最近有成功内镜治疗的病例报道。在此,我们阐明了内镜干预对延迟穿孔患者的有效性。
评估2005年至2022年接受胃ESD的患者是否符合条件。延迟穿孔定义为ESD术后无术中穿孔,但随后在计算机断层扫描上出现腹膜刺激征和游离气体。根据聚乙醇酸(PGA)片和套扎器(OTSC)在临床实践中的应用时间(2015年10月)将参与者分为早期组和晚期组。我们评估了所需手术发生率的变化。
在5048例接受胃ESD的患者中,28例发生延迟穿孔(0.6%,95%置信区间[CI]0.4%-0.8%)。早期组和晚期组延迟穿孔的发生率无显著差异(0.5%对0.6%)。晚期组接受手术的患者比例显著低于早期组(54%对13%,优势比[OR]0.14,95%CI 0.02-0.83;P=0.042);在对年龄、性别、Charlson合并症指数、肿瘤位置和大小进行调整后,多因素分析证实了这一点(调整后的OR 0.04,95%CI 0.002-0.9;P=0.043)。
使用PGA片和OTSC的内镜干预与胃ESD后延迟穿孔所需手术的低发生率相关,因此推荐使用。