Asare Amma, Previs Rebecca Ann, Spinosa Daniel, Fellman Bryan, Scott Amelia L, Mulder Isabelle, Mahmoud May, Enbaya Ahmed, Siedel Jean Hansen, Cobb Lauren, Soliman Pamela T, Sood Anil K, Coleman Robert L, Secord Angeles Alvarez, Westin Shannon N
Department of Gynecologic Oncology & Reproductive Medicine, The University of Texas MD Anderson Cancer Center, United States of America.
LabCorp, Chapel Hill, NC, United States of America.
Gynecol Oncol. 2025 Mar;194:112-118. doi: 10.1016/j.ygyno.2025.02.015. Epub 2025 Feb 22.
This study evaluated whether patients with epithelial ovarian, fallopian tube, and primary peritoneal carcinoma (OC) who are immediately re-treated with bevacizumab derive benefit after disease progression on a bevacizumab-containing regimen.
This multi-institutional, retrospective study compared patients with high grade non-mucinous epithelial OC who received bevacizumab followed directly by another bevacizumab-containing treatment regimen to patients who received bevacizumab followed by a regimen that did not contain bevacizumab (or received no further treatment). Progression-free survival (PFS) and overall survival (OS) were estimated using Kaplan Meier product-limit estimator and modeled via Cox proportional hazards regression.
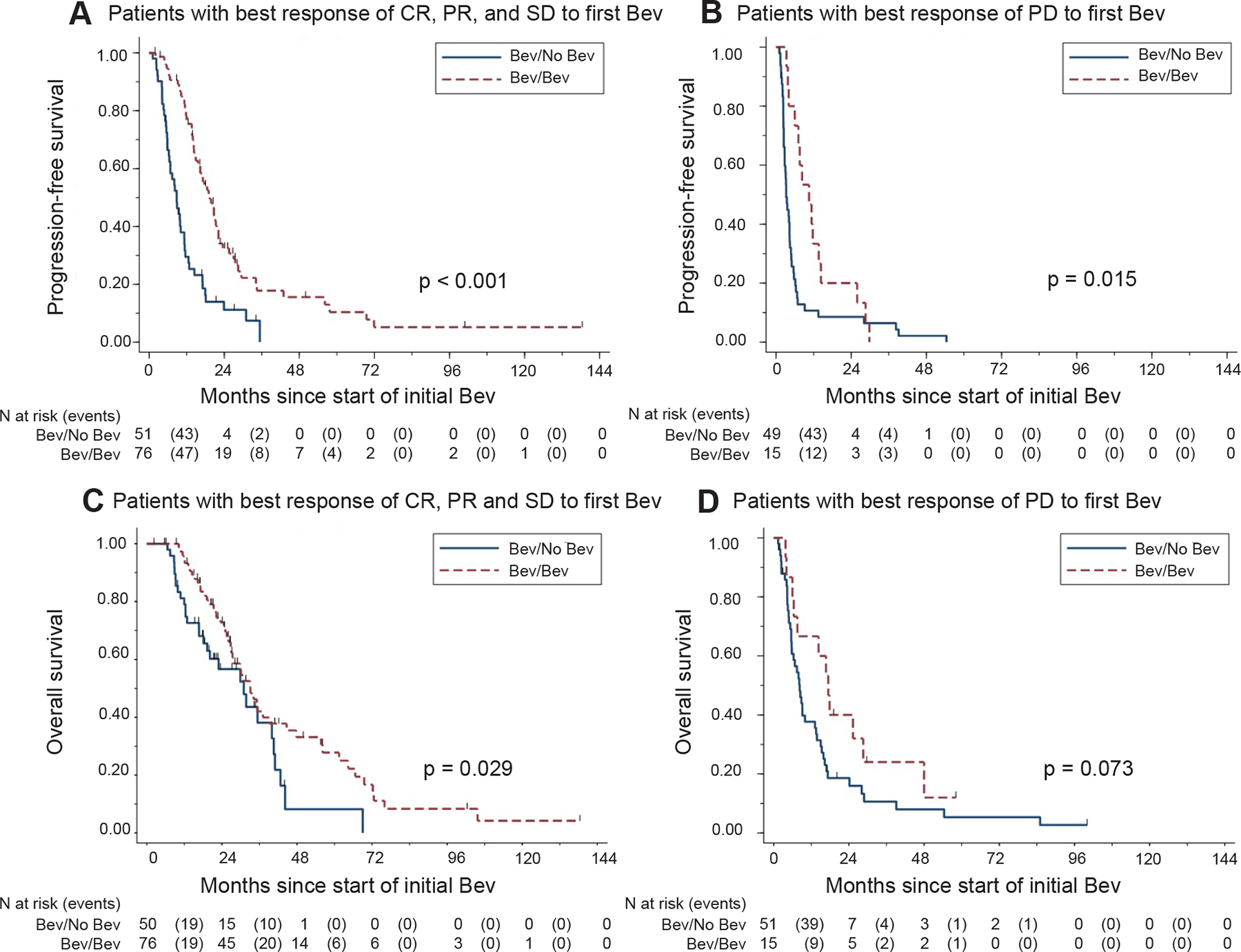
Among 226 patients with OC who received bevacizumab as part of a treatment regimen,103 received sequential treatment with bevacizumab and 123 received a bevacizumab-containing regimen followed by a non-bevacizumab-containing regimen at the time of progression. Median follow-up for all subjects was 17.3 months (range, 1.2-138.2 months). Median PFS was 17.2 months (95 % CI, 14.3-21.2) for patients who received sequential bevacizumab re-treatment and 5.1 months (95 % CI, 4.3-6.3) for patients who received bevacizumab without bevacizumab-containing re-treatment (p < 0.001). Median OS was 29.9 months (95 % CI, 26.1-35.4) for patients who received sequential bevacizumab re-treatment (p < 0.001) and 12.4 months (95 % CI, 9.2-16.7) for patients who did not receive bevacizumab-containing re-treatment.
Patients with OC treated with bevacizumab-containing regimens sequentially at the time of progression have prolonged survival compared to patients who received no re-treatment with bevacizumab.
本研究评估了上皮性卵巢癌、输卵管癌和原发性腹膜癌(OC)患者在含贝伐单抗方案疾病进展后立即再次接受贝伐单抗治疗是否有益。
这项多机构回顾性研究将接受贝伐单抗治疗后直接接受另一种含贝伐单抗治疗方案的高级别非黏液性上皮性OC患者与接受贝伐单抗治疗后接受不含贝伐单抗方案(或未接受进一步治疗)的患者进行了比较。无进展生存期(PFS)和总生存期(OS)采用Kaplan-Meier乘积限估计法进行估计,并通过Cox比例风险回归进行建模。
在226例接受贝伐单抗作为治疗方案一部分的OC患者中,103例接受了贝伐单抗序贯治疗,123例在疾病进展时接受了含贝伐单抗方案治疗,随后接受了不含贝伐单抗的方案治疗。所有受试者的中位随访时间为17.3个月(范围1.2-138.2个月)。接受贝伐单抗序贯再治疗的患者中位PFS为17.2个月(95%CI,14.3-21.2),接受贝伐单抗治疗但未接受含贝伐单抗再治疗的患者中位PFS为5.1个月(95%CI,4.3-6.3)(p<0.001)。接受贝伐单抗序贯再治疗的患者中位OS为29.9个月(95%CI,26.1-35.4)(p<0.001),未接受含贝伐单抗再治疗的患者中位OS为12.4个月(95%CI,9.2-16.7)。
与未接受贝伐单抗再治疗的患者相比,进展时接受含贝伐单抗方案序贯治疗的OC患者生存期延长。