Elmeliegy Mohamed, Viqueira Andrea, Vandendries Erik, Hickman Anne, Conte Umberto, Irby Donald, Hibma Jennifer, Lon Hoi-Kei, Piscitelli Joseph, Soltantabar Pooneh, Skoura Athanasia, Jiang Sibo, Wang Diane
Oncology Research and Development, Pfizer Inc., San Diego, CA, 92121, USA.
Oncology Research and Development, Pfizer SLU, Madrid, Spain.
Target Oncol. 2025 Mar;20(2):349-359. doi: 10.1007/s11523-025-01134-8. Epub 2025 Feb 25.
Elranatamab is a BCMA-CD3 bispecific antibody approved for the treatment of relapsed or refractory multiple myeloma. Cytokine release syndrome is one of the most common adverse events associated with bispecific antibodies.
We aimed to determine the optimal elranatamab dosing regimen for mitigating cytokine release syndrome.
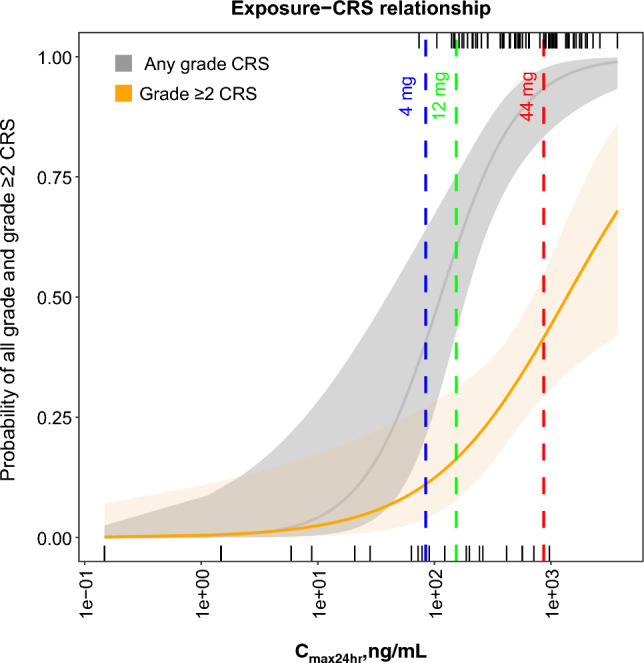
Safety, pharmacokinetics, and exposure-response were analyzed across four clinical studies (MagnetisMM-1, MagnetisMM-2, MagnetisMM-3, and MagnetisMM-9). Different priming regimens evaluated across these studies included a one-step-up dose priming regimen of 44 mg with or without premedication, a two-step-up dose priming regimen of 12 mg on day 1 and 32 mg on day 4 with premedication, and a two-step-up dose priming regimen of 4 mg on day 1 and 20 mg on day 4 with premedication.
The maximum elranatamab serum concentration on day 1 was positively associated with any-grade and grade ≥ 2 cytokine release syndrome. A slower time to maximum serum concentration and a lower dose-normalized maximum serum concentration were observed with subcutaneous versus intravenous administration, supporting subcutaneous dosing to help mitigate cytokine release syndrome.
Based on the incidence, severity, and predictable profile of cytokine release syndrome, the 12/32-mg priming-dose regimen with premedication was determined to be the optimal regimen before the first full dose of 76 mg on day 8.
ClinicalTrials.gov identifiers: NCT03269136, NCT04798586, NCT04649359, and NCT05014412.
埃拉纳单抗是一种获批用于治疗复发或难治性多发性骨髓瘤的BCMA-CD3双特异性抗体。细胞因子释放综合征是与双特异性抗体相关的最常见不良事件之一。
我们旨在确定减轻细胞因子释放综合征的最佳埃拉纳单抗给药方案。
对四项临床研究(MagnetisMM-1、MagnetisMM-2、MagnetisMM-3和MagnetisMM-9)的安全性、药代动力学和暴露-反应进行了分析。这些研究中评估的不同启动方案包括44 mg的一步递增剂量启动方案(有或无预处理)、第1天12 mg和第4天32 mg并进行预处理的两步递增剂量启动方案,以及第1天4 mg和第4天20 mg并进行预处理的两步递增剂量启动方案。
第1天的埃拉纳单抗血清最大浓度与任何级别和≥2级细胞因子释放综合征呈正相关。与静脉给药相比,皮下给药观察到达到血清最大浓度的时间较慢且剂量标准化的血清最大浓度较低,这支持皮下给药有助于减轻细胞因子释放综合征。
基于细胞因子释放综合征的发生率、严重程度和可预测特征,在第8天首次给予76 mg全剂量之前,确定12/32 mg启动剂量并进行预处理的方案为最佳方案。
ClinicalTrials.gov标识符:NCT03269136、NCT04798586、NCT04649359和NCT05014412。