Liu Xiaoqiang, Wang Yubin, Huang Yingxuan, Lin Chanchan, Xu Boming, Zeng Yilin, Chen Peizhong, Liu Xiaobo, Huang Yisen
Department of Gastroenterology, First Hospital of Quanzhou Affiliated to Fujian Medical University, Quanzhou, Fujian, China.
McConnell Brain Imaging Centre, Montreal Neurological Institute, McGill University, Montreal, QC, Canada.
BMC Cancer. 2025 Feb 25;25(1):338. doi: 10.1186/s12885-025-13760-6.
Cancer survivors may experience accelerated biological aging, increasing their risk of mortality. However, the association between phenotypic age acceleration (PAA) and mortality among cancer survivors remains unclear. This study aimed to evaluate the relationship between PAA and all-cause mortality, cancer-specific mortality, and non-cancer mortality among adult cancer survivors in the United States.
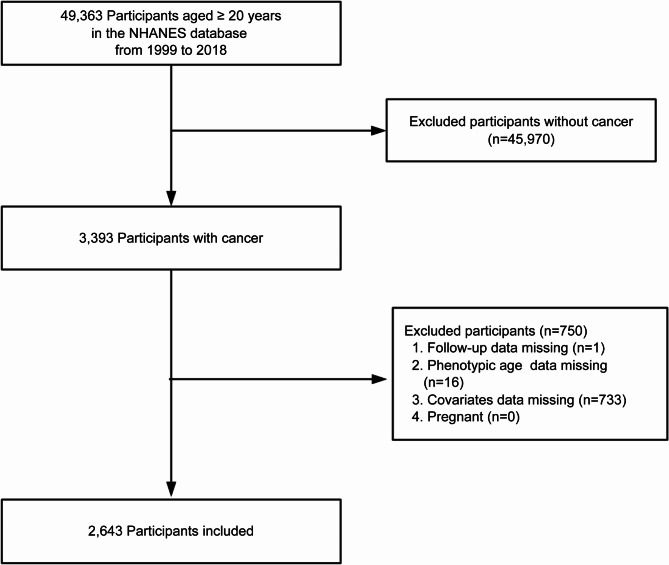
We utilized data from the National Health and Nutrition Examination Survey (NHANES) from 1999 to 2018, including 2,643 (unweighted) cancer patients aged ≥ 20 years. Phenotypic age was calculated using ten physiological biomarkers, and the residuals from regressing phenotypic age on chronological age (age acceleration residuals, AAR) were used to determine PAA status. Participants were divided into PAA and without PAA groups based on the sign of the residuals. Weighted Cox proportional hazards regression models were used to assess the association between PAA and mortality, adjusting for demographic characteristics, lifestyle factors, and comorbidities. Restricted cubic spline (RCS) models were employed to explore the dose-response relationship between AAR and mortality.
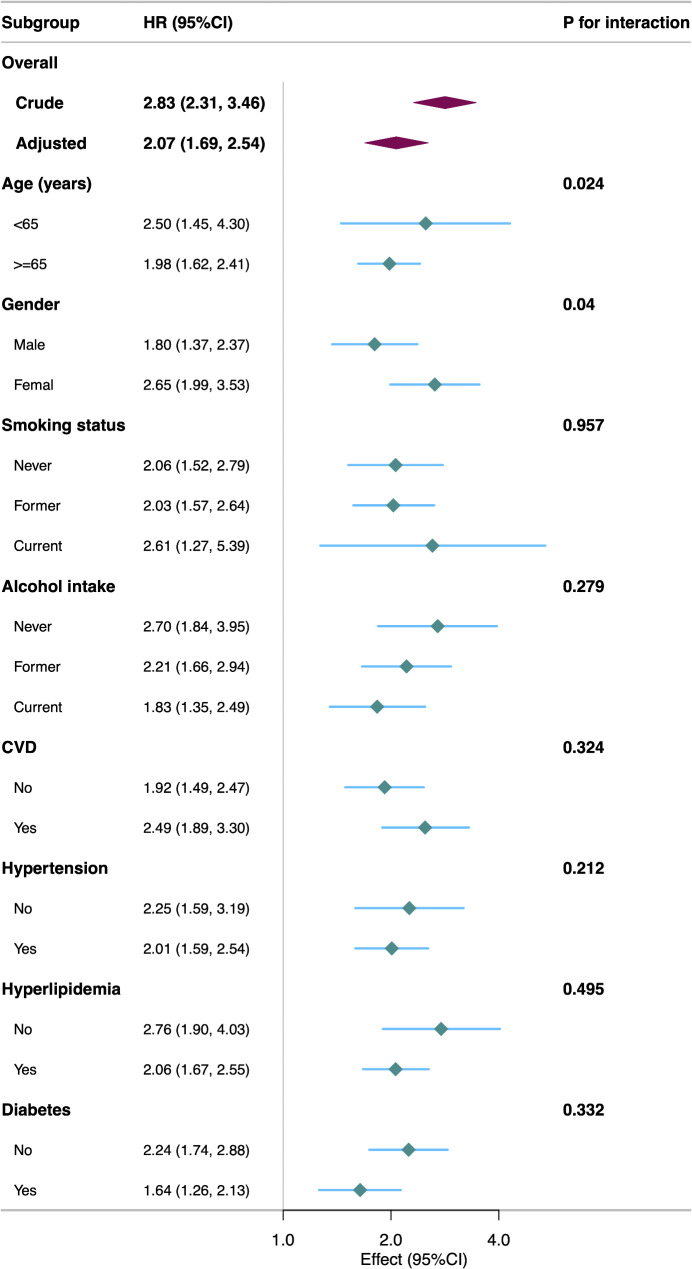
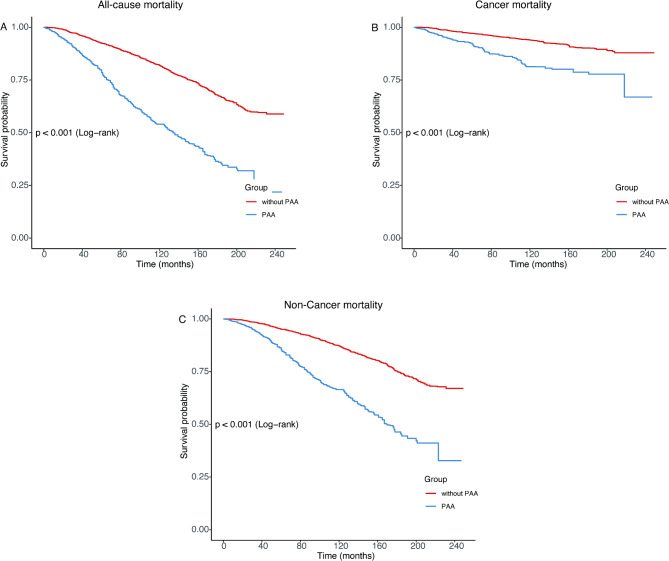
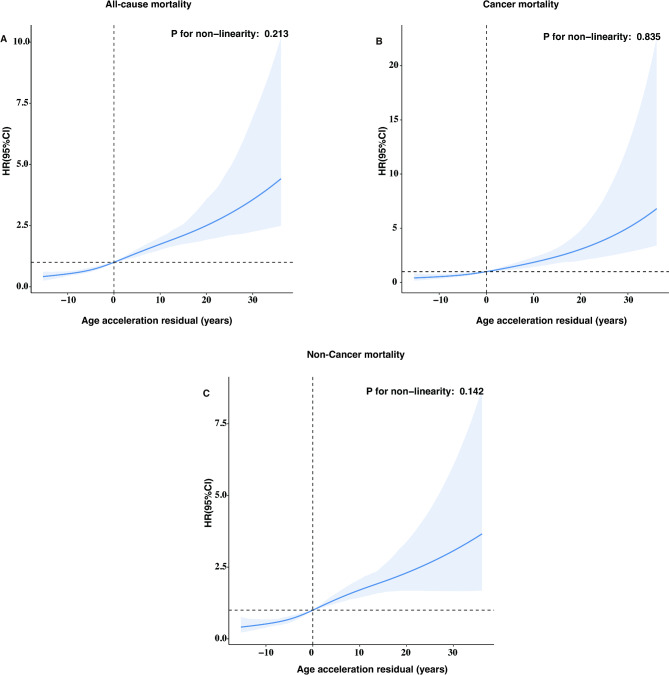
Over a median follow-up of 9.16 years, 991 (unweighted) participants died. After adjusting for multiple covariates, PAA was significantly associated with increased risks of all-cause mortality (HR = 2.07; 95% CI: 1.69-2.54), cancer-specific mortality (HR = 2.15; 95% CI: 1.52-3.04), and non-cancer mortality (HR = 2.06; 95% CI: 1.66-2.57). Each one-unit increase in AAR was associated with a 4% increase in the risk of all-cause, cancer-specific, and non-cancer mortality (HR = 1.04; 95% CI: 1.03-1.05). RCS models indicated a linear dose-response relationship between AAR and mortality.
Among U.S. adult cancer survivors, PAA is significantly associated with all-cause, cancer-specific, and non-cancer mortality. PAA may serve as an important biomarker for predicting prognosis in cancer survivors.
癌症幸存者可能经历生物衰老加速,增加其死亡风险。然而,癌症幸存者的表型年龄加速(PAA)与死亡率之间的关联仍不明确。本研究旨在评估美国成年癌症幸存者中PAA与全因死亡率、癌症特异性死亡率和非癌症死亡率之间的关系。
我们利用了1999年至2018年美国国家健康与营养检查调查(NHANES)的数据,其中包括2643名(未加权)年龄≥20岁的癌症患者。使用十种生理生物标志物计算表型年龄,并将表型年龄对实足年龄进行回归得到的残差(年龄加速残差,AAR)用于确定PAA状态。根据残差的符号将参与者分为PAA组和无PAA组。使用加权Cox比例风险回归模型评估PAA与死亡率之间的关联,并对人口统计学特征、生活方式因素和合并症进行调整。采用受限立方样条(RCS)模型探索AAR与死亡率之间的剂量反应关系。
在中位随访9.16年期间,991名(未加权)参与者死亡。在调整多个协变量后,PAA与全因死亡率(HR = 2.07;95%CI:1.69 - 2.54)、癌症特异性死亡率(HR = 2.15;95%CI:1.52 - 3.04)和非癌症死亡率(HR = 2.06;95%CI:1.66 - 2.57)的风险增加显著相关。AAR每增加一个单位,全因、癌症特异性和非癌症死亡率的风险增加4%(HR = 1.04;95%CI:1.03 - 1.05)。RCS模型表明AAR与死亡率之间存在线性剂量反应关系。
在美国成年癌症幸存者中,PAA与全因、癌症特异性和非癌症死亡率显著相关。PAA可能作为预测癌症幸存者预后的重要生物标志物。