Liu Ying, Yin Xuejun, Guo Yutong, Xu Jixiong, Shao Ruitai, Kong Yunyuan
Department of Emergency, The First Affiliated Hospital, Jiangxi Medical College, Nanchang University, Nanchang, People's Republic of China.
School of Population Medicine and Public Health, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People's Republic of China.
BMC Pulm Med. 2025 Feb 26;25(1):90. doi: 10.1186/s12890-025-03525-z.
Respiratory sarcopenia is associated with poor outcomes, yet effective biomarkers for risk stratification remain limited. This study investigates the associations between complete blood count (CBC)-derived inflammatory biomarkers, including neutrophil-to-lymphocyte ratio (NLR), neutrophil-monocyte-to-lymphocyte ratio (NMLR), and systemic inflammation response index (SIRI) and both all-cause and cardiovascular mortality in patients with respiratory sarcopenia.
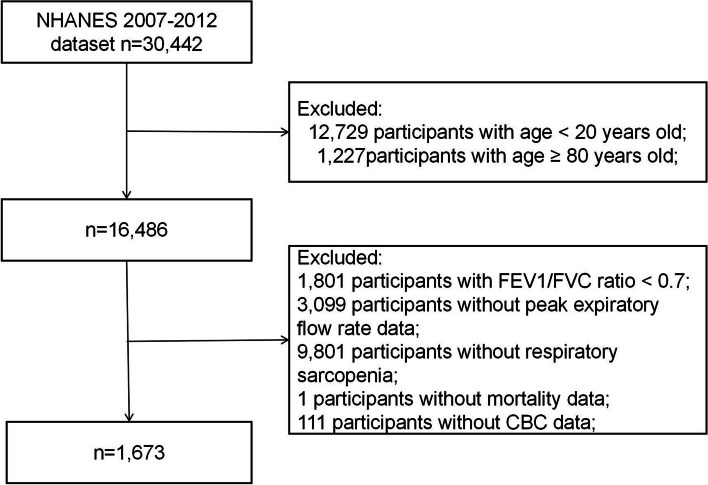
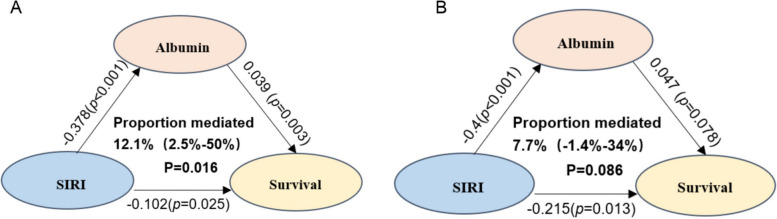
We conducted a cohort analysis of 1,673 adults with possible respiratory sarcopenia using data from the National Health and Nutrition Examination Survey (NHANES) from 2007 to 2012, with mortality follow-up through December 31, 2019. Possible respiratory sarcopenia was assessed via peak expiratory flow rate (PEFR). Multivariable Cox regression models evaluated associations between NLR, NMLR, SIRI, and mortality outcomes, adjusted for demographic, socioeconomic, and health-related covariates. Additional CBC-derived biomarkers (PLR, dNLR, MLR, SII) were analysed, and mediation analysis assessed albumin's role as a partial mediator of mortality.
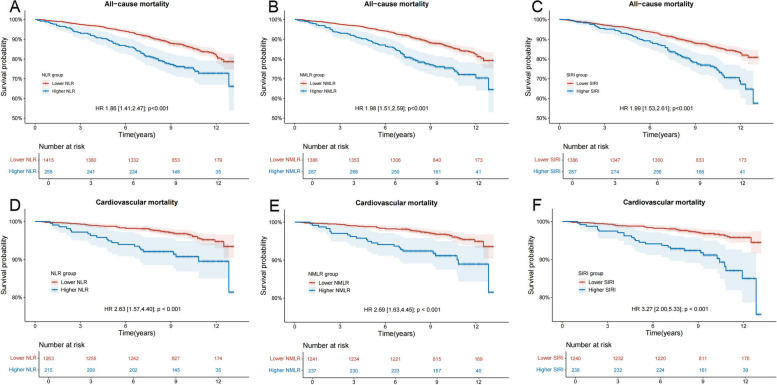
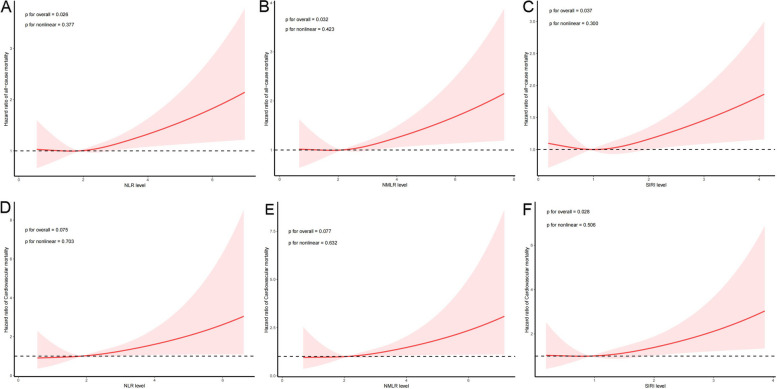
Over a median follow-up of 116 months, 263 deaths occurred, including 68 from cardiovascular causes. Elevated NLR, NMLR, and SIRI were significantly associated with increased risks of all-cause and cardiovascular mortality. SIRI emerged as the strongest predictor, with adjusted hazard ratios (HRs) of 1.65 (95% CI, 1.23-2.22) for all-cause mortality and 3.18 (95% CI, 1.83-5.53) for cardiovascular mortality. Albumin partially mediated the relationship between SIRI and all-cause mortality (12.1%).
Elevated NLR, NMLR, and SIRI are associated with increased mortality risks in respiratory sarcopenia, with SIRI demonstrating the highest predictive power. Integrating SIRI into clinical assessments may aid in identifying high-risk patients, allowing for targeted interventions.
呼吸肌减少症与不良预后相关,但用于风险分层的有效生物标志物仍然有限。本研究调查了全血细胞计数(CBC)衍生的炎症生物标志物,包括中性粒细胞与淋巴细胞比值(NLR)、中性粒细胞 - 单核细胞与淋巴细胞比值(NMLR)以及全身炎症反应指数(SIRI)与呼吸肌减少症患者全因死亡率和心血管死亡率之间的关联。
我们使用2007年至2012年美国国家健康和营养检查调查(NHANES)的数据,对1673名可能患有呼吸肌减少症的成年人进行了队列分析,并对截至2019年12月31日的死亡率进行了随访。通过呼气峰值流速(PEFR)评估可能的呼吸肌减少症。多变量Cox回归模型评估了NLR、NMLR、SIRI与死亡率结局之间的关联,并对人口统计学、社会经济和健康相关协变量进行了调整。分析了其他CBC衍生的生物标志物(PLR、dNLR、MLR、SII),并通过中介分析评估白蛋白作为死亡率部分中介的作用。
在中位随访116个月期间,发生了263例死亡,其中68例死于心血管原因。NLR、NMLR和SIRI升高与全因死亡率和心血管死亡率增加显著相关。SIRI是最强的预测因子,全因死亡率的调整后风险比(HR)为1.65(95%CI,1.23 - 2.22),心血管死亡率的调整后HR为3.18(95%CI,1.83 - 5.53)。白蛋白部分介导了SIRI与全因死亡率之间的关系(12.1%)。
NLR、NMLR和SIRI升高与呼吸肌减少症患者的死亡风险增加相关,其中SIRI显示出最高的预测能力。将SIRI纳入临床评估可能有助于识别高危患者,从而进行有针对性的干预。