Espinoza Diego A, Zrzavy Tobias, Breville Gautier, Thebault Simon, Marefi Amaar, Mexhitaj Ina, Kan Mengyuan, Bacchus Micky, Legaspi Jessica, Fernandez Samantha, Melamed Anna, Stubblebine Mallory, Kim Yeseul, Martinez Zachary, Diorio Caroline, Schulte-Mecklenbeck Andreas, Wiendl Heinz, Rezk Ayman, Li Rui, Narula Sona, Waldman Amy T, Hopkins Sarah E, Banwell Brenda, Bar-Or Amit
Center for Neuroinflammation and Experimental Therapeutics, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA.
Department of Neurology, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA.
bioRxiv. 2025 Mar 1:2025.02.27.637541. doi: 10.1101/2025.02.27.637541.
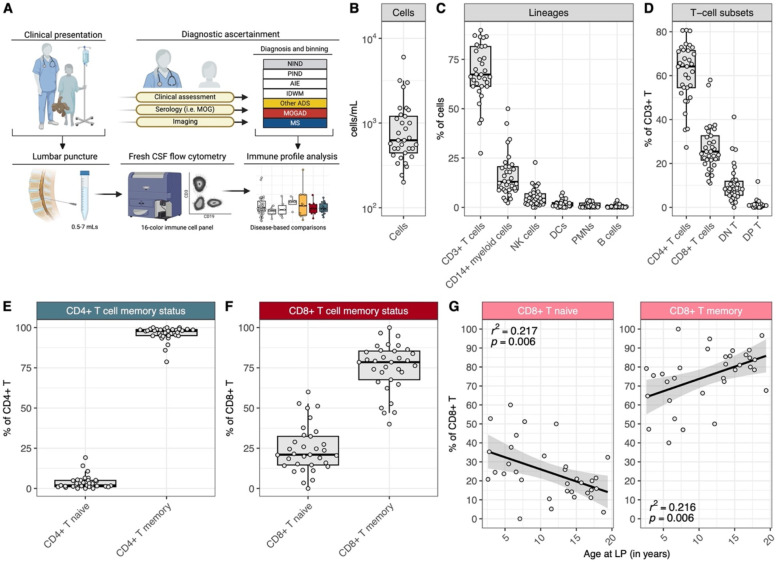
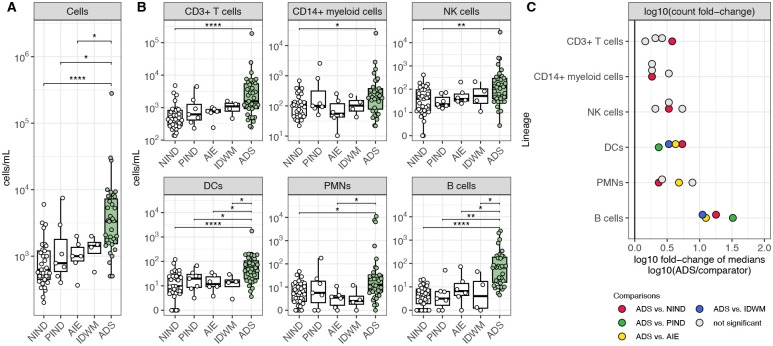
The cerebrospinal fluid (CSF) provides a unique glimpse into the central nervous system (CNS) compartment and offers insights into immune processes associated with both healthy immune surveillance as well as inflammatory disorders of the CNS. The latter include demyelinating disorders, such as multiple sclerosis (MS) and myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD), that warrant different therapeutic approaches yet are not always straightforward to distinguish on clinical and imaging grounds alone. Here, we establish a comprehensive phenotypic landscape of the pediatric CSF immune compartment across a range of non-inflammatory and inflammatory neurological disorders, with a focus on better elucidating CNS-associated immune mechanisms potentially involved in, and discriminating between, pediatric-onset MS (MS) and other pediatric-onset suspected neuroimmune disorders, including MOGAD. We find that CSF from pediatric patients with non-inflammatory neurological disorders is primarily composed of non-activated CD4+ T cells, with few if any B cells present. CSF from pediatric patients with acquired inflammatory demyelinating disorders is characterized by increased numbers of B cells compared to CSF of both patients with other inflammatory or non-inflammatory conditions. Certain features, including particular increased frequencies of antibody-secreting cells (ASCs) and decreased frequencies of CD14+ myeloid cells, distinguish MS from MOGAD and other acquired inflammatory demyelinating disorders.
脑脊液(CSF)为了解中枢神经系统(CNS)区室提供了独特视角,并有助于深入了解与健康免疫监测以及中枢神经系统炎症性疾病相关的免疫过程。后者包括脱髓鞘疾病,如多发性硬化症(MS)和髓鞘少突胶质细胞糖蛋白抗体相关疾病(MOGAD),这些疾病需要不同的治疗方法,但仅根据临床和影像学依据并不总是容易区分。在此,我们建立了一系列非炎症性和炎症性神经系统疾病中儿童脑脊液免疫区室的综合表型图谱,重点是更好地阐明可能参与儿童期多发性硬化症(MS)和其他儿童期疑似神经免疫疾病(包括MOGAD)并对其进行区分的中枢神经系统相关免疫机制。我们发现,患有非炎症性神经系统疾病的儿童患者的脑脊液主要由未激活的CD4+T细胞组成,几乎没有B细胞。与患有其他炎症或非炎症性疾病的患者的脑脊液相比,患有获得性炎症性脱髓鞘疾病的儿童患者的脑脊液具有B细胞数量增加的特征。某些特征,包括抗体分泌细胞(ASC)的特定频率增加和CD14+髓样细胞的频率降低,可将MS与MOGAD和其他获得性炎症性脱髓鞘疾病区分开来。