Sousa Mayson L A, Menga Luca S, Schreiber Annia, Docci Mattia, Vieira Fernando, Katira Bhushan H, Pellegrini Mariangela, Dubo Sebastian, Douflé Ghislaine, Costa Eduardo L V, Post Martin, Amato Marcelo B P, Brochard Laurent
Keenan Centre for Biomedical Research, Li Ka Shing Knowledge Institute, St. Michael's Hospital, Unity Health Toronto, Toronto, Canada.
Interdepartmental Division of Critical Care Medicine, University of Toronto, Toronto, Canada.
Crit Care. 2025 Mar 10;29(1):107. doi: 10.1186/s13054-025-05325-7.
There are several approaches to select the optimal positive end-expiratory pressure (PEEP), resulting in different PEEP levels. The impact of different PEEP settings may extend beyond respiratory mechanics, affecting pulmonary hemodynamics.
To compare PEEP levels obtained with three titration strategies-(i) highest respiratory system compliance (C), (ii) electrical impedance tomography (EIT) crossing point; (iii) positive end-expiratory transpulmonary pressure (P)-in terms of regional respiratory mechanics and pulmonary hemodynamics.
Experimental studies in two porcine models of acute lung injury: (I) bilateral injury induced in both lungs, generating a highly recruitable model (n = 37); (II) asymmetrical injury, generating a poorly recruitable model (n = 13). In all experiments, a decremental PEEP titration was performed monitoring P, EIT (collapse, overdistention, and regional ventilation), respiratory mechanics, and pulmonary and systemic hemodynamics.
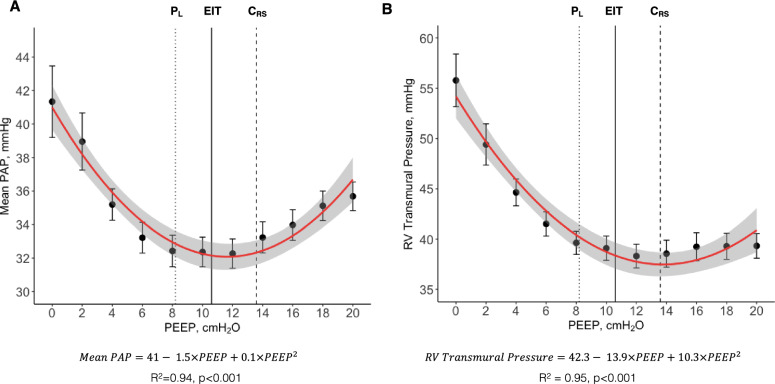
PEEP titration methods resulted in different levels of median optimal PEEP in bilateral lung injury: 14(12-14) cmHO for C, 11(10-12) cmHO for EIT, and 8(8-10) cmHO for P, p < 0.001. Differences were less pronounced in asymmetrical lung injury. PEEP had a quadratic U-shape relationship with pulmonary artery pressure (R = 0.94, p < 0.001), right-ventricular systolic transmural pressure, and pulmonary vascular resistance. Minimum values of pulmonary vascular resistance were found around individualized PEEP, when ventilation distribution and pulmonary circulation were simultaneously optimized.
In porcine models of acute lung injury with variable lung recruitability, both low and high levels of PEEP can impair pulmonary hemodynamics. Optimized ventilation and hemodynamics can be obtained simultaneously at PEEP levels individualized based on respiratory mechanics, especially by EIT and esophageal pressure.
有多种方法来选择最佳呼气末正压(PEEP),从而导致不同的PEEP水平。不同PEEP设置的影响可能不仅限于呼吸力学,还会影响肺血流动力学。
比较通过三种滴定策略获得的PEEP水平——(i)最高呼吸系统顺应性(C);(ii)电阻抗断层扫描(EIT)交叉点;(iii)呼气末跨肺压(P)——在局部呼吸力学和肺血流动力学方面的差异。
在两个急性肺损伤猪模型中进行实验研究:(I)双侧肺损伤,构建一个易于复张的模型(n = 37);(II)不对称损伤,构建一个难以复张的模型(n = 13)。在所有实验中,进行递减式PEEP滴定,监测P、EIT(肺萎陷、过度扩张和局部通气)、呼吸力学以及肺和全身血流动力学。
在双侧肺损伤中,PEEP滴定方法导致不同水平的中位最佳PEEP:C法为14(12 - 14)cmH₂O,EIT法为11(10 - 12)cmH₂O,P法为8(8 - 10)cmH₂O,p < 0.001。在不对称肺损伤中差异不太明显。PEEP与肺动脉压(R = 0.94,p < 0.001)、右心室收缩跨壁压和肺血管阻力呈二次U形关系。当通气分布和肺循环同时优化时,在个体化PEEP附近发现肺血管阻力的最小值。
在肺复张能力不同的急性肺损伤猪模型中,低水平和高水平的PEEP均可能损害肺血流动力学。基于呼吸力学,尤其是通过EIT和食管压力个体化的PEEP水平,可以同时实现优化的通气和血流动力学。