Djalalinia Shirin, Khosravi Sepehr, Yoosefi Moein, Salahi Sarvenaz, Varniab Zahra Shokri, Golestani Ali, Rezaei Nazila, Kazemi Ameneh, Dilmaghani-Marand Arezou, Rezaei Negar, Ghasemi Erfan, Ahmadi Naser, Rashidi Mohammad-Mahdi, Farzi Yosef, Rezaee Kamyar, Nasserinejad Maryam, Azadnajafabad Sina, Abdolhamidi Elham, Haghshenas Rosa, Derouei Arefeh Alipour, Rankohi Azadeh Momen Nia, Farzadfar Farshad
Non-Communicable Diseases Research Center, Endocrinology and Metabolism Population Sciences Institute, Tehran University of Medical Sciences, Second Floor, No.10, Jalal Al-E-Ahmad Highway, Tehran, 1411713137, Iran.
Development of Research and Technology Center, Deputy of Research and Technology Ministry of Health and Medical Education, Tehran, Iran.
Lipids Health Dis. 2025 Mar 18;24(1):99. doi: 10.1186/s12944-025-02506-9.
Noncommunicable diseases (NCDs), particularly cardiovascular disease (CVD), are the leading cause of death worldwide, with hypercholesterolemia being a major risk factor for CVD. This study evaluated the hypercholesterolemia care cascade in Iran-including prevalence, diagnosis, treatment coverage, and effectiveness-using the National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP III) guidelines.
This cross-sectional study drew on data from the 2021 Iran STEPS survey, which employed a systematic cluster sampling of adults aged ≥ 18 years across all provinces in Iran. Hypercholesterolemia was defined per NCEP-ATP III thresholds (LDL ≥ 160 mg/dL, total cholesterol ≥ 240 mg/dL, HDL ≤ 40 mg/dL, or ongoing lipid-lowering therapy). Weighted descriptive statistics were calculated, and Poisson regression with robust variance estimated crude and adjusted prevalence ratios for optimal lipid control among those treated. The 10-year CVD risk was determined using the Framingham Risk Score, stratifying participants into low (< 10%), intermediate (10-20%), and high (> 20%) risk categories.
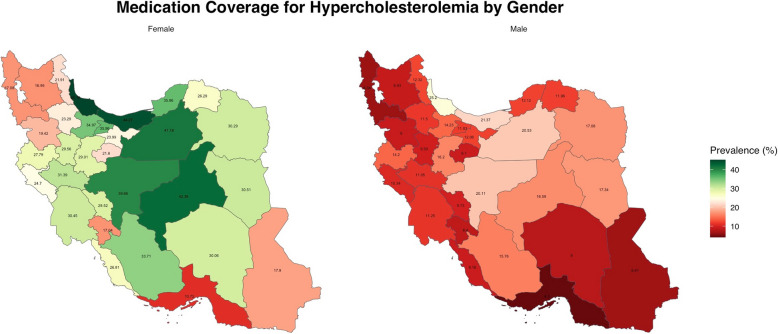
Out of 18,074 participants, 10,582 (55.32%, 95% CI: 54.29-56.35) met NCEP-ATP III criteria for hypercholesterolemia. Among these, only 20.61% (19.55-21.72) were receiving pharmacological treatment. Treatment coverage was notably lower in males (13.15%, 11.98-14.40) than females (29.12%, 27.35-30.96). Statins were the most commonly used medication (11.43% of males, 25.87% of females). Of those receiving treatment, 52.85% (females) and 53.93% (males) achieved optimal LDL, while 76.98% (females) and 81.06% (males) attained total cholesterol < 200 mg/dL. However, only 19.89% (females) and 3.97% (males) met the HDL > 60 mg/dL goal. The 10-year CVD risk was < 10% in 57.79% of participants, 10-20% in 33.27%, and > 20% in 8.94%.
Despite a high prevalence of hypercholesterolemia in Iran, treatment coverage remains suboptimal, particularly among males and working-age adults. Although most treated individuals achieve favorable LDL and total cholesterol levels, gaps persist in achieving optimal HDL targets. These findings underscore the need for strengthened screening, treatment, and adherence strategies-alongside broader preventive measures-to reduce the burden of hypercholesterolemia and CVD in Iran.
非传染性疾病(NCDs),尤其是心血管疾病(CVD),是全球主要的死亡原因,高胆固醇血症是心血管疾病的主要危险因素。本研究使用美国国家胆固醇教育计划成人治疗小组第三次报告(NCEP-ATP III)指南,评估了伊朗的高胆固醇血症治疗流程,包括患病率、诊断、治疗覆盖率和有效性。
这项横断面研究利用了2021年伊朗STEP调查的数据,该调查对伊朗所有省份年龄≥18岁的成年人采用了系统整群抽样。高胆固醇血症根据NCEP-ATP III阈值定义(低密度脂蛋白≥160mg/dL、总胆固醇≥240mg/dL、高密度脂蛋白≤40mg/dL或正在进行降脂治疗)。计算加权描述性统计量,并使用稳健方差的泊松回归估计治疗人群中最佳血脂控制的粗患病率和调整患病率比值。使用弗明汉风险评分确定10年心血管疾病风险,将参与者分为低风险(<10%)、中风险(10-20%)和高风险(>20%)类别。
在18074名参与者中,10582人(55.32%,95%CI:54.29-56.35)符合NCEP-ATP III高胆固醇血症标准。其中,只有20.61%(19.55-21.72)正在接受药物治疗。男性的治疗覆盖率(13.15%,11.98-14.40)明显低于女性(29.12%,27.35-30.96)。他汀类药物是最常用的药物(男性为11.43%,女性为25.87%)。在接受治疗的人中,52.85%(女性)和53.93%(男性)的低密度脂蛋白达到最佳水平,而76.98%(女性)和81.06%(男性)的总胆固醇<200mg/dL。然而,只有19.89%(女性)和3.97%(男性)达到高密度脂蛋白>60mg/dL的目标。57.79%的参与者10年心血管疾病风险<10%,33.27%为10-20%,8.94%>20%。
尽管伊朗高胆固醇血症患病率很高,但治疗覆盖率仍不理想,尤其是在男性和工作年龄成年人中。虽然大多数接受治疗的个体低密度脂蛋白和总胆固醇水平良好,但在实现最佳高密度脂蛋白目标方面仍存在差距。这些发现强调需要加强筛查、治疗和依从性策略,以及更广泛的预防措施,以减轻伊朗高胆固醇血症和心血管疾病的负担。