Farina Antonio, Villagrán-García Macarena, Abichou-Klich Amna, Benaiteau Marie, Bernard Emilien, Campetella Lucia, Cluse Florent, Desestret Virginie, Dumez Pauline, Fabien Nicole, Goncalves David, Muñiz-Castrillo Sergio, Picard Géraldine, Pinto Anne-Laurie, Rogemond Véronique, Vogrig Alberto, Joubert Bastien, Honnorat Jérôme
French Reference Centre on Paraneoplastic Neurological Syndromes and Autoimmune Encephalitis, Hospices Civils de Lyon, Hôpital Neurologique, 59 Boulevard Pinel, 69677, Bron Cedex, France.
MeLiS-UCBL-CNRS UMR 5284, INSERM U1314, Université Claude Bernard Lyon 1, Lyon, France.
J Neurol. 2025 Mar 19;272(4):273. doi: 10.1007/s00415-025-13001-7.
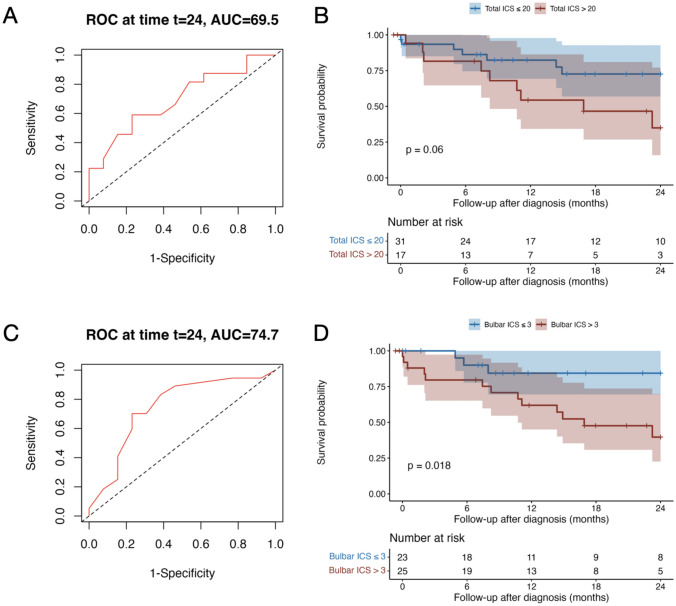
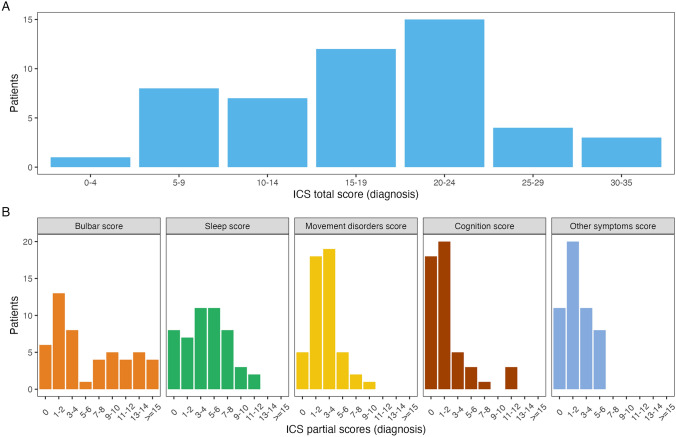
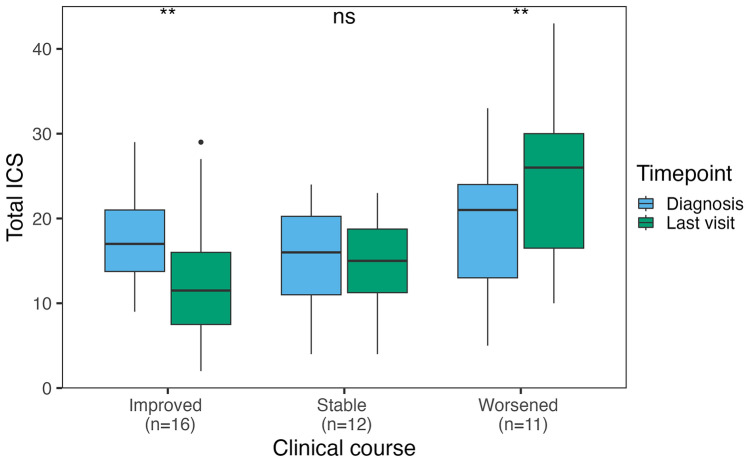
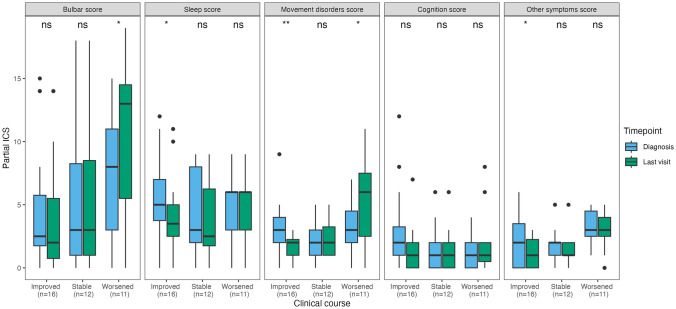
Anti-IgLON5 disease presents with diverse symptoms, whose severity can be measured by the anti-IgLON5 disease composite score (ICS). This study applied the ICS to a retrospective anti-IgLON5 disease cohort (n = 52; median age 72 years, 63% male) diagnosed in the French Reference Center on Autoimmune Encephalitis (2016-2024), aiming to describe severity and clinical course, and to assess its potential to predict mortality. At diagnosis, the ICS distribution (median 18) aligned with previous publications and correlated with the time to diagnosis (median 19 months); all patients had symptoms in ≥ 2 ICS domains: bulbar (88%), sleep (84%), movement disorders (90%), cognition (64%), and/or other (78%). Of 46 patients with follow-up data, 7 (16%) died shortly after diagnosis; for the others, changes in the ICS mirrored the clinical course: at last visit, it decreased in improving patients (16/46, 35%; median 12 vs 17; p = 0.004), increased in worsening patients (11/39, 24%; median 26 vs 21; p = 0.006) and did not change significantly in stable patients (12/46, 26%; median 16 vs 15; p = 0.222). In the ROC analyses, 2-year mortality was predicted by the total ICS at diagnosis (AUC 69.51, 95% CI [50.19; 88.83]; optimal cut-off > 20, sensitivity 59%, specificity 77%), and by the bulbar score at diagnosis (AUC 74.68, 95% CI [56.17, 93.19]; optimal cut-off > 3, sensitivity 83%, specificity 62%). The ICS is a reproducible tool for assessing anti-IgLON5 disease severity and clinical course. Higher total and bulbar ICS at diagnosis are associated with increased mortality risk, underscoring the need for early and intensive management of bulbar dysfunction.
抗IgLON5疾病表现出多种症状,其严重程度可通过抗IgLON5疾病综合评分(ICS)来衡量。本研究将ICS应用于在法国自身免疫性脑炎参考中心(2016 - 2024年)诊断的抗IgLON5疾病回顾性队列(n = 52;中位年龄72岁,63%为男性),旨在描述疾病严重程度和临床病程,并评估其预测死亡率的潜力。诊断时,ICS分布(中位数为18)与先前发表的结果一致,且与诊断时间(中位数为19个月)相关;所有患者在≥2个ICS领域有症状:延髓(88%)、睡眠(84%)、运动障碍(90%)、认知(64%)和/或其他(78%)。在46例有随访数据的患者中,7例(16%)在诊断后不久死亡;对于其他患者,ICS的变化反映了临床病程:在最后一次就诊时,病情改善的患者ICS降低(16/46,35%;中位数12对17;p = 0.004),病情恶化的患者ICS升高(11/39,24%;中位数26对21;p = 0.006),病情稳定的患者ICS无显著变化(12/46,26%;中位数16对15;p = 0.222)。在ROC分析中,诊断时的总ICS可预测2年死亡率(AUC 69.51,95% CI [50.19;88.83];最佳截断值>20,敏感性59%,特异性77%),诊断时的延髓评分也可预测(AUC 74.68,95% CI [56.17,93.19];最佳截断值>3,敏感性83%,特异性62%)。ICS是评估抗IgLON5疾病严重程度和临床病程的可重复工具。诊断时较高的总ICS和延髓ICS与死亡风险增加相关,强调了对延髓功能障碍进行早期和强化管理的必要性。