Yang Luwei, Fan Guihua, Zhang Lijuan, Zhou Binbin, Dai Xiaomin, Ji Zongfei, Ma Lingying, Zhang Zhuojun, Chen Huiyong, Yu Qiang, Ma Lili, Jiang Lindi, Sun Ying
Department of Rheumatology, Zhongshan Hospital (Xiamen), Fudan University, Xiamen, China.
Department of Rheumatology, Zhongshan Hospital, Fudan University, Shanghai, China.
Front Immunol. 2025 Mar 5;16:1471152. doi: 10.3389/fimmu.2025.1471152. eCollection 2025.
Infection is a leading cause of mortality in idiopathic inflammatory myopathies (IIMs). This study aimed to develop a nomogram for predicting severe infection risk in IIM patients.
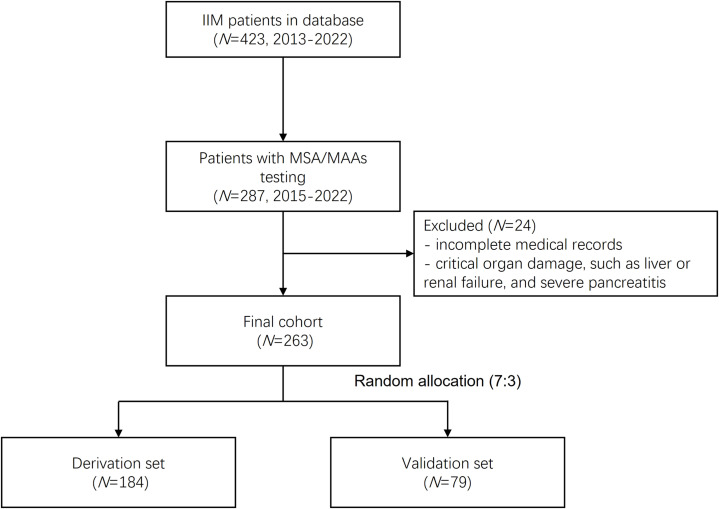
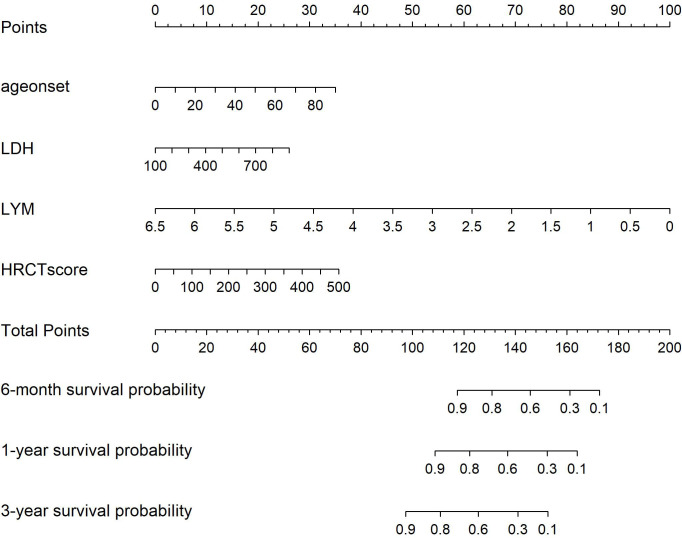
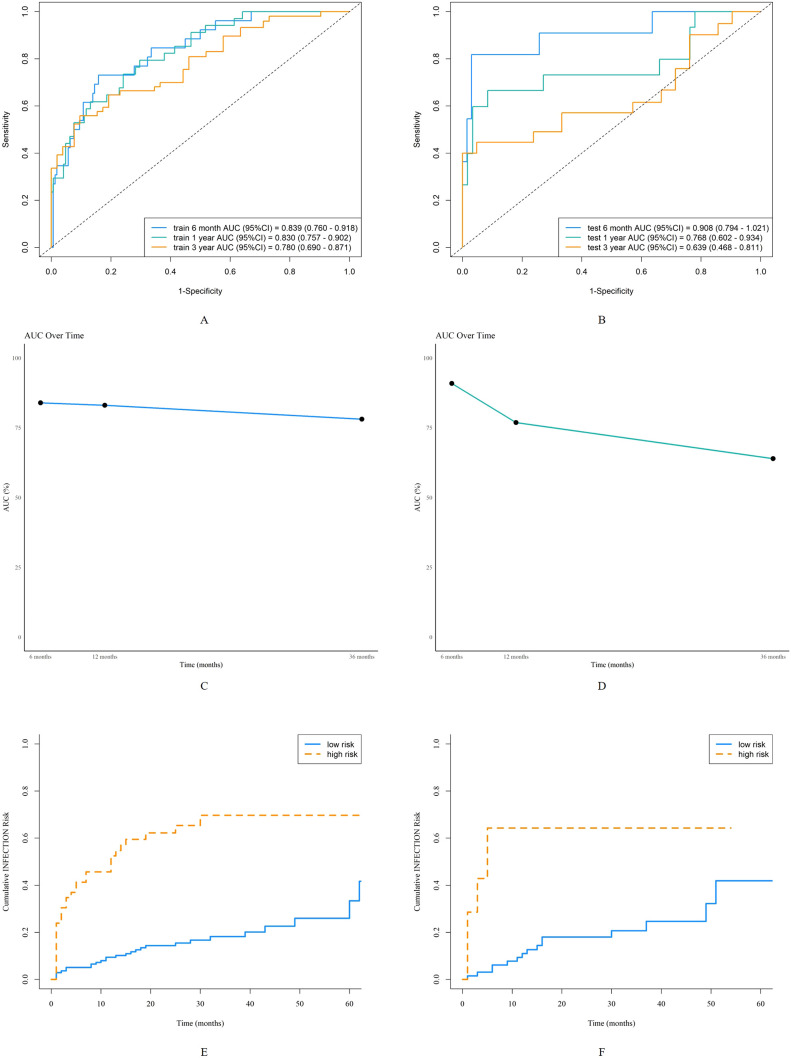
Patients with IIMs admitted to Zhongshan Hospital, Fudan University, from January 2015 to January 2022 were enrolled. They were randomly divided into derivation (70%) and validation (30%) sets. Univariate and multivariate Cox regression identified independent risk factors for severe infection, and the Akaike information criterion (AIC) was applied for model selection. A nomogram was constructed to predict severe infection risks at 6 months, 1 year, and 3 years. Predictive accuracy and discriminative ability were evaluated using the concordance index (C-index), calibration curves, and the area under the receiver operating characteristic curve (AUC). Decision curve analysis (DCA) assessed clinical utility. Kaplan-Meier (K-M) curves were used to analyze survival differences between high- and low-risk groups stratified by nomogram scores.
Among 263 IIM patients, 81 experienced 106 severe infection events, with lower respiratory tract infections being the most common (47.2%). Independent risk factors included age at onset (HR 1.024, 95% CI 1.002-1.046, =0.036), lactate dehydrogenase (HR 1.002, 95% CI 0.999-1.005, =0.078), HRCT score (HR 1.004, 95% CI 1.001-1.006, =0.002), and lymphocyte count (HR 0.48, 95% CI 0.23-0.99, =0.048). The nomogram demonstrated strong predictive performance, with AUCs of 0.84, 0.83, and 0.78 for 6 months, 1 year, and 3 years in the derivation set, and 0.91, 0.77, and 0.64 in the validation set. Calibration curves showed good agreement between predicted and observed risks, while DCA demonstrated significant net benefit over individual predictors. Kaplan-Meier curves revealed significant differences in the cumulative risk of severe infection between high- and low-risk groups. Further validation in DM and ASS subgroups demonstrated that the nomogram effectively predicted severe infections, with AUCs of 0.86, 0.81, and 0.73 for DM and 0.86, 0.83, and 0.74 for ASS at 6 months, 1 year, and 3 years, respectively.
We have developed a new nomogram to predict severe infection risk in IIM patients at 6 months, 1 year, and 3 years. This model aids clinicians and patients in formulating treatment and follow-up strategies.
感染是特发性炎症性肌病(IIM)患者死亡的主要原因。本研究旨在开发一种列线图,用于预测IIM患者发生严重感染的风险。
纳入2015年1月至2022年1月在复旦大学附属中山医院住院的IIM患者。将他们随机分为推导组(70%)和验证组(30%)。单因素和多因素Cox回归确定严重感染的独立危险因素,并应用赤池信息准则(AIC)进行模型选择。构建列线图以预测6个月、1年和3年时的严重感染风险。使用一致性指数(C指数)、校准曲线和受试者工作特征曲线下面积(AUC)评估预测准确性和判别能力。决策曲线分析(DCA)评估临床实用性。采用Kaplan-Meier(K-M)曲线分析按列线图评分分层的高风险组和低风险组之间的生存差异。
在263例IIM患者中,81例发生了106次严重感染事件,其中下呼吸道感染最为常见(47.2%)。独立危险因素包括发病年龄(HR 1.024,95%CI 1.002-1.046,P=0.036)、乳酸脱氢酶(HR 1.002,95%CI 0.999-1.005,P=0.078)、HRCT评分(HR 1.004,95%CI 1.001-1.006,P=0.002)和淋巴细胞计数(HR 0.48,95%CI 0.23-0.99,P=0.048)。列线图显示出强大的预测性能,推导组中6个月、1年和3年的AUC分别为0.84、0.83和0.78,验证组中分别为0.91、0.77和0.64。校准曲线显示预测风险与观察到的风险之间具有良好的一致性,而DCA显示出比个体预测指标更大的净效益。Kaplan-Meier曲线显示高风险组和低风险组之间严重感染的累积风险存在显著差异。在皮肌炎(DM)和抗合成酶综合征(ASS)亚组中的进一步验证表明,列线图能有效预测严重感染,DM组在6个月、1年和3年时的AUC分别为0.86、0.81和0.73,ASS组分别为0.86、0.83和0.74。
我们开发了一种新的列线图,用于预测IIM患者在6个月、1年和3年时发生严重感染的风险。该模型有助于临床医生和患者制定治疗和随访策略。