Dura Ilknur Cinar, Dura Mustafa Cengiz, Tosun Miğraci, Çelik Handan, Arslan Hatice Nilden, Kökçü Arif
Obstetrics and Gynaecology, Ondokuz Mayıs University Faculty of Medicine, Samsun, TUR.
Obstetrics and Gynaecology, Bakırköy Sadi Konuk Education and Research Hospital, Istanbul, TUR.
Cureus. 2025 Feb 24;17(2):e79575. doi: 10.7759/cureus.79575. eCollection 2025 Feb.
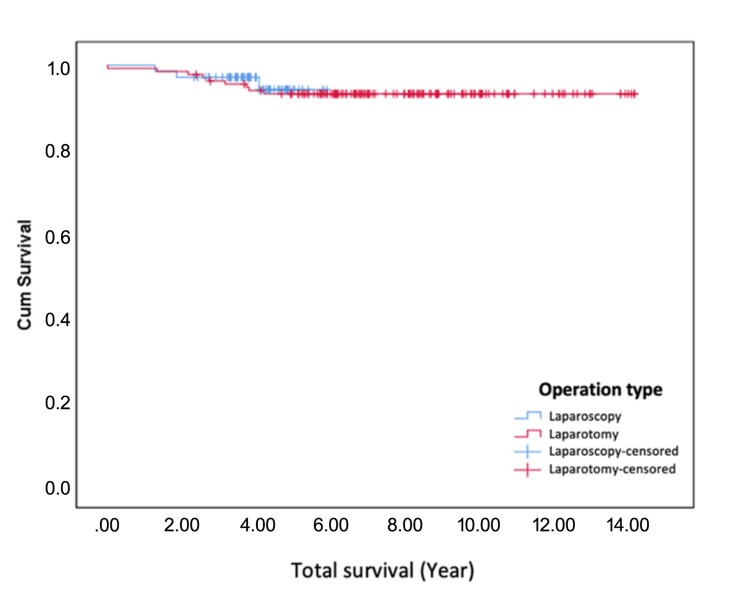
Objective This study aims to compare the surgical and postoperative outcomes, as well as the safety and efficacy, of laparoscopic surgery and laparotomy in patients diagnosed with early-stage endometrioid endometrial cancer, focusing on operative time, intraoperative blood transfusion requirements, postoperative complications, and recurrence rates. Materials and methods Data were collected on patients who underwent surgery at the Department of Obstetrics and Gynaecology, Ondokuz Mayıs University Faculty of Medicine, with a diagnosis of endometrial cancer between January 2007 and December 2018. Patients were assessed using the staging approach proposed by FIGO in 2009. Patients with endometrioid adenocarcinoma histology in stages IA, IB, and II were chosen; 69 underwent laparoscopic surgery, and 133 underwent laparotomy. Patient survival rates, cancer recurrence, demographic information, and intraoperative and postoperative outcomes were compared. Results There was no significant difference between the groups in terms of survival and disease-free survival. The tumor size was larger in the laparotomy group, which may be attributed to preoperative imaging and clinical assessment guiding the surgical approach. The laparoscopy group had a shorter postoperative hospital stay, required less intraoperative blood transfusion, and experienced fewer postoperative complications. However, the operation time was shorter in the laparotomy group, likely due to the technical complexity of laparoscopy, which typically requires longer preparation and instrument handling times. While laparoscopy provides magnification that enhances visualization and access to lymph nodes, the number of pelvic and total lymph nodes removed was higher in the laparotomy group, possibly reflecting the standard surgical approach used in open procedures. These outcomes were compared and evaluated between the two surgical methods. All surgeries were performed by surgeons with similar levels of expertise in both techniques. Discussion Although the duration of the laparoscopy method is long, it has advantages such as short hospital stay, less intraoperative blood requirement, fewer post-operative complications, and early return to daily activities. There is no difference between both methods in terms of cancer recurrence and survival. The mean, 5-year survival and disease-free survival of the patients were similar. Conclusion Laparoscopic surgery is as safe and effective as laparotomy in the treatment of early-stage endometrial cancer. While this study reinforces an already well-established fact, it is important to acknowledge the continuous advancements in minimally invasive surgical techniques, including robotic surgery and vaginal natural orifice transluminal endoscopic surgery (vNOTES). Future research should focus on comparing these emerging techniques to further refine surgical approaches and optimize patient outcomes.
目的 本研究旨在比较腹腔镜手术与开腹手术在早期子宫内膜样腺癌患者中的手术及术后结果,以及安全性和有效性,重点关注手术时间、术中输血需求、术后并发症及复发率。
材料与方法 收集2007年1月至2018年12月在翁多库兹迈伊斯大学医学院妇产科接受手术且诊断为子宫内膜癌的患者数据。采用国际妇产科联盟(FIGO)2009年提出的分期方法对患者进行评估。选取IA期、IB期和II期子宫内膜样腺癌组织学类型的患者;69例行腹腔镜手术,133例行开腹手术。比较患者生存率、癌症复发情况、人口统计学信息以及术中及术后结果。
结果 两组在生存率和无病生存率方面无显著差异。开腹手术组肿瘤体积较大,这可能归因于术前影像学检查和临床评估对手术方式的指导。腹腔镜手术组术后住院时间较短,术中输血需求较少,术后并发症较少。然而,开腹手术组手术时间较短,可能是由于腹腔镜手术技术复杂,通常需要更长的准备时间和器械操作时间。虽然腹腔镜手术提供放大功能,可增强可视化并便于获取淋巴结,但开腹手术组切除的盆腔淋巴结和总淋巴结数量较多,这可能反映了开放手术中使用的标准手术方式。对两种手术方法的这些结果进行了比较和评估。所有手术均由在两种技术方面专业水平相似的外科医生进行。
讨论 虽然腹腔镜手术方法耗时较长,但具有住院时间短、术中输血需求少、术后并发症少以及能早期恢复日常活动等优点。两种方法在癌症复发和生存率方面无差异。患者的平均、5年生存率和无病生存率相似。
结论 在早期子宫内膜癌的治疗中,腹腔镜手术与开腹手术一样安全有效。虽然本研究强化了一个已确立的事实,但必须承认微创外科技术在不断进步,包括机器人手术和经阴道自然腔道内镜手术(vNOTES)。未来的研究应侧重于比较这些新兴技术,以进一步完善手术方式并优化患者预后。
