Karaca Irmak, Bromeo Albert John, Mobasserian Azadeh, Akhavanrezayat Amir, DeBoer Charles, Thng Zheng Xian, Hung Jia-Horung, Yoo Woong-Sun, Khatri Anadi, Yavari Negin, Nguyen Ba Trung, El Feky Dalia, Yasar Cigdem, Elaraby Osama, Saengsirinavin Aim-On, Zhang Xiaoyan, Anover Frances Andrea, Gupta Ankur Sudhir, Do Diana V, Or Christopher, Nguyen Quan Dong
Spencer Center for Vision Research, Byers Eye Institute, School of Medicine, Stanford University, 2370 Watson Court, Palo Alto, CA, USA.
Moran Eye Center, University of Utah, Salt Lake City, UT, USA.
J Ophthalmic Inflamm Infect. 2025 Mar 27;15(1):34. doi: 10.1186/s12348-025-00459-9.
To report IgG4-related ophthalmic disease (IgG4-ROD) presenting as posterior scleritis in a pediatric patient.
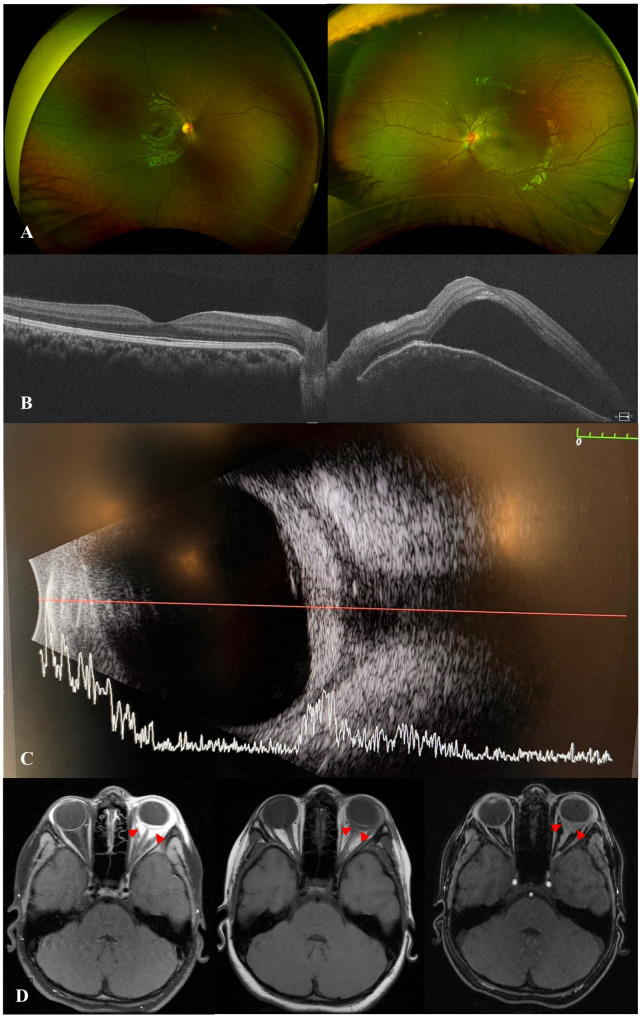
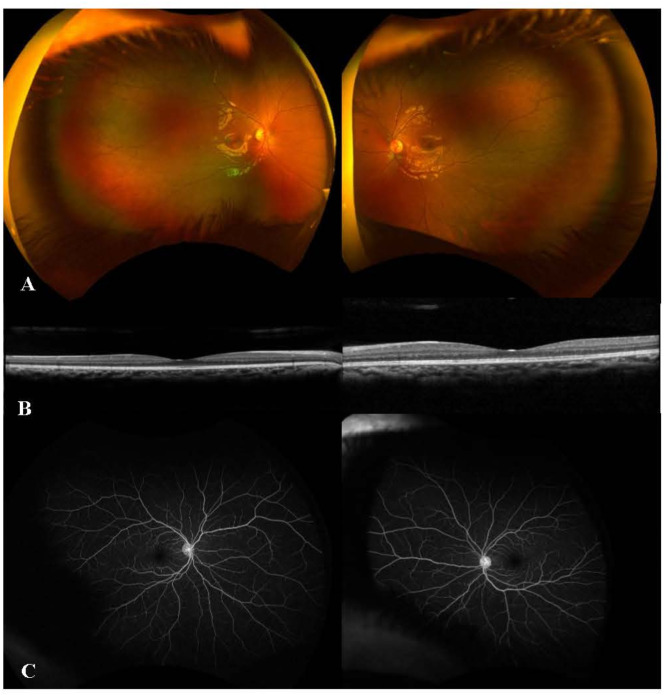
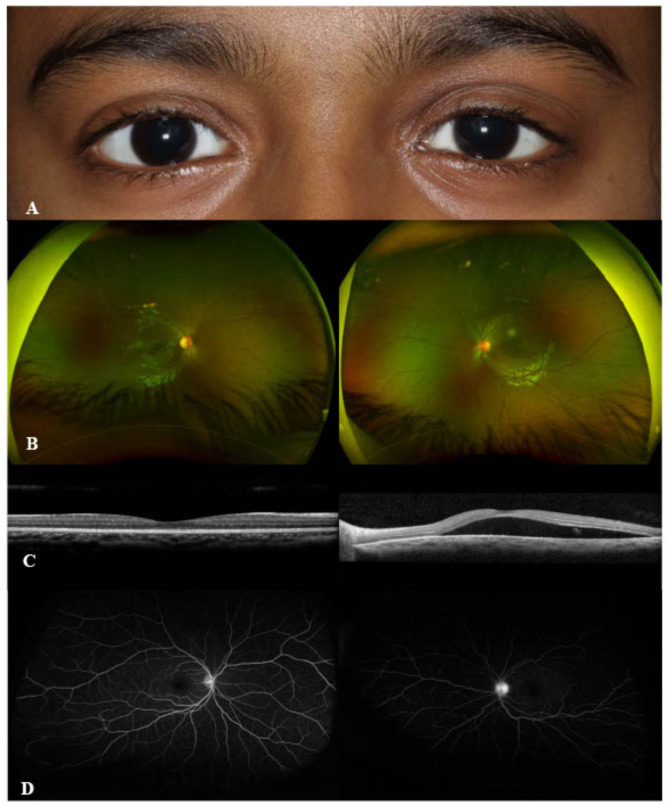
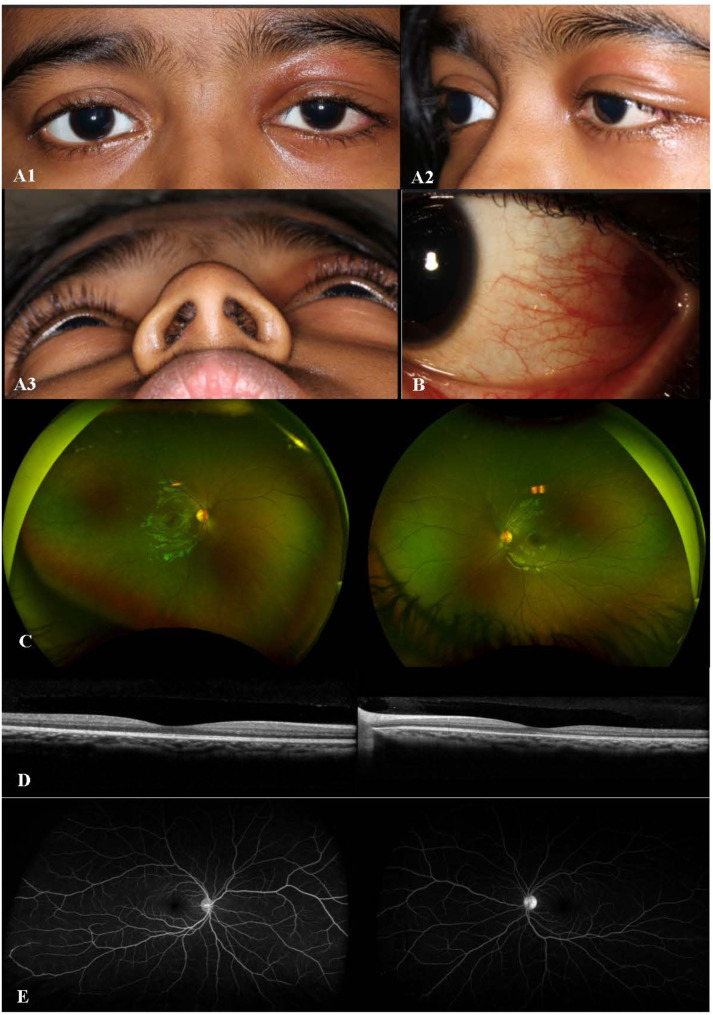
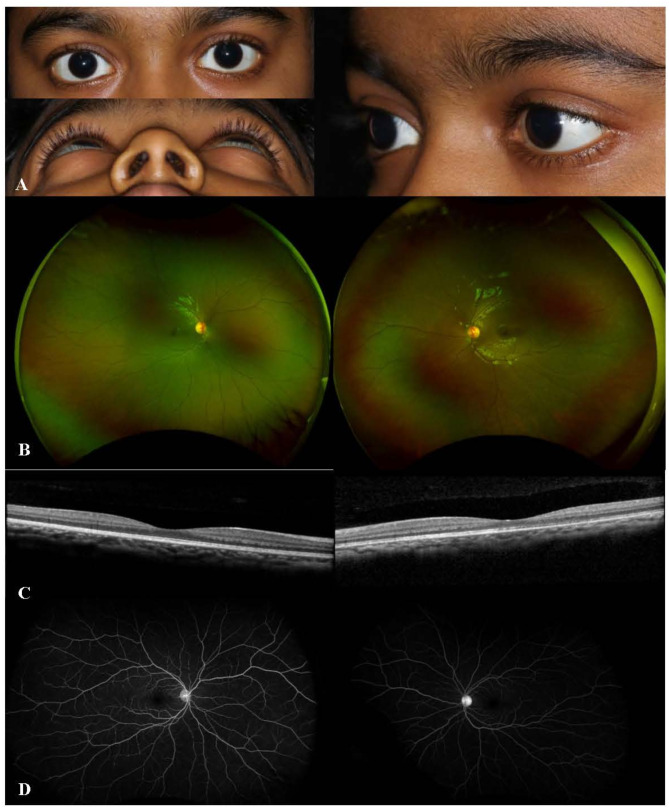
A 7-year-old girl presented with proptosis, painful eyelid swelling, and restricted extraocular movements (EOM) of her left eye (OS). Visual acuity (VA) was 20/20 in right eye (OD) and counting fingers (CF) at 1 foot in OS. Slit lamp examination revealed 2 + anterior chamber (AC) cells, optic disc edema (ODE) with elevated appearance of macula in OS. Optical coherence tomography (OCT) showed significant subretinal fluid (SRF) in macula, B-scan ultrasound (US) demonstrated T-sign in OS. Orbital MRI was also consistent with posterior scleritis and periorbital inflammation. Extensive systemic work-up was unremarkable. Thus, the patient was started on intravenous methylprednisolone (IVMP) 30 mg/kg/day for 3 days, along with topical therapy in OS, which led to an improvement of proptosis, EOM restriction, AC cells, as well as ODE and SRF in macula in OS. Fluorescein angiography (FA) showed leakage from optic disc in OS. The patient was then switched to oral prednisone with slow tapering and started on methotrexate (MTX). Given the recurrence of proptosis and painful eyelid swelling on systemic steroid tapering, serum IgG4 levels were ordered and found to be elevated at 149.9 mg/dL (range, 1-99). Therefore, the patient was diagnosed as 'possible' IgG4-ROD (based on diagnostic criteria) and started on infliximab (7.5 mg/kg) and IVMP monthly infusions with continuation of MTX 20 mg weekly and slower tapering of oral prednisone, which led to resolution of clinical findings, improvement of VA to 20/20 in OS.
Posterior scleritis may be the initial presentation of IgG4-ROD in children. Refractory course is not uncommon. Biologics are effective in the long-term control of inflammation.
报告1例以儿童后巩膜炎形式表现的IgG4相关性眼病(IgG4-ROD)。
一名7岁女孩出现左眼(OS)眼球突出、眼睑疼痛性肿胀及眼球运动(EOM)受限。右眼(OD)视力(VA)为20/20,OS为眼前1英尺数指(CF)。裂隙灯检查显示OS前房(AC)细胞2+、视盘水肿(ODE)伴黄斑外观隆起。光学相干断层扫描(OCT)显示黄斑区有大量视网膜下液(SRF),B超(US)显示OS有T征。眼眶MRI也与后巩膜炎及眶周炎症相符。全面的系统检查无异常。因此,患者开始静脉注射甲泼尼龙(IVMP)30mg/kg/天,共3天,同时对OS进行局部治疗,这使OS的眼球突出、EOM受限、AC细胞以及黄斑区的ODE和SRF得到改善。荧光素血管造影(FA)显示OS视盘渗漏。然后患者改用口服泼尼松并逐渐减量,并开始使用甲氨蝶呤(MTX)。鉴于全身用类固醇逐渐减量时眼球突出和眼睑疼痛性肿胀复发,检测血清IgG4水平,发现升高至149.9mg/dL(范围1-99)。因此,根据诊断标准,该患者被诊断为“可能的”IgG4-ROD,并开始使用英夫利昔单抗(7.5mg/kg)及每月静脉注射IVMP,继续每周使用MTX 20mg并更缓慢地减少口服泼尼松剂量,这使临床症状消退,OS的VA提高至20/20。
后巩膜炎可能是儿童IgG4-ROD的初始表现。难治性病程并不少见。生物制剂对长期控制炎症有效。