Baumeister Hannah, Gellersen Helena M, Polk Sarah E, Lattmann René, Wuestefeld Anika, Wisse Laura E M, Glenn Trevor, Yakupov Renat, Stark Melina, Kleineidam Luca, Roeske Sandra, Morgado Barbara Marcos, Esselmann Hermann, Brosseron Frederic, Ramirez Alfredo, Lüsebrink Falk, Synofzik Matthis, Schott Björn H, Schmid Matthias C, Hetzer Stefan, Dechent Peter, Scheffler Klaus, Ewers Michael, Hellmann-Regen Julian, Ersözlü Ersin, Spruth Eike, Gemenetzi Maria, Fliessbach Klaus, Bartels Claudia, Rostamzadeh Ayda, Glanz Wenzel, Incesoy Enise I, Janowitz Daniel, Rauchmann Boris-Stephan, Kilimann Ingo, Sodenkamp Sebastian, Coenjaerts Marie, Spottke Annika, Peters Oliver, Priller Josef, Schneider Anja, Wiltfang Jens, Buerger Katharina, Perneczky Robert, Teipel Stefan, Laske Christoph, Wagner Michael, Ziegler Gabriel, Jessen Frank, Düzel Emrah, Berron David
German Center for Neurodegenerative Diseases (DZNE), Magdeburg, Germany.
Cognition and Brain Sciences Unit, University of Cambridge, Cambridge, United Kingdom.
medRxiv. 2025 Mar 14:2025.03.13.25323904. doi: 10.1101/2025.03.13.25323904.
Structural MRI often lacks diagnostic, prognostic, and monitoring value in Alzheimer's disease (AD), particularly in early disease stages. To improve its utility, we aimed to identify optimal MRI readouts for different use cases.
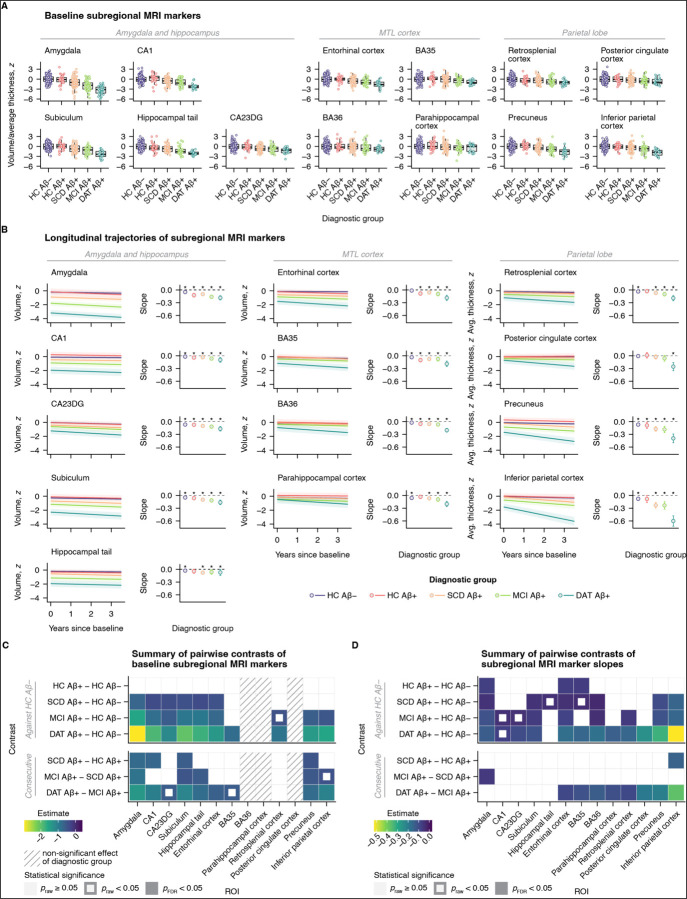
We included 363 older adults; healthy controls (HC) who were negative or positive for amyloidbeta (Aβ) and Aβ-positive patients with subjective cognitive decline (SCD), mild cognitive impairment, or dementia of the Alzheimer type. MRI and neuropsychological assessments were administered annually for up to three years.
Accelerated atrophy of distinct MTL subregions was evident already during preclinical AD. Symptomatic disease stages most notably differed in their hippocampal and parietal atrophy signatures. Associations of atrophy markers and cognitive inventories varied by intended use and disease stage.
With the appropriate readout, MRI can detect abnormal atrophy already during preclinical AD. To optimize performance, MRI readouts should be tailored to the targeted disease stage and intended use.
结构磁共振成像(MRI)在阿尔茨海默病(AD)中通常缺乏诊断、预后和监测价值,尤其是在疾病早期阶段。为了提高其效用,我们旨在确定针对不同应用场景的最佳MRI读数。
我们纳入了363名老年人;淀粉样蛋白β(Aβ)阴性或阳性的健康对照(HC)以及Aβ阳性的主观认知下降(SCD)、轻度认知障碍或阿尔茨海默型痴呆患者。每年进行MRI和神经心理学评估,最长持续三年。
在临床前AD阶段,不同内侧颞叶(MTL)亚区域的加速萎缩就已很明显。有症状的疾病阶段在海马体和顶叶萎缩特征方面差异最为显著。萎缩标志物与认知量表的关联因预期用途和疾病阶段而异。
通过适当的读数,MRI在临床前AD阶段就能检测到异常萎缩。为了优化性能,MRI读数应根据目标疾病阶段和预期用途进行定制。