Zhang Xi-Ru, Zhong Wen-Fang, Liu Rui-Yan, Huang Jie-Lin, Fu Jing-Xiang, Gao Jian, Zhang Pei-Dong, Liu Dan, Li Zhi-Hao, He Yan, Zhou Hongwei, Li Zhuang
Microbiome Medicine Center, Department of Laboratory Medicine, Zhujiang Hospital, Southern Medical University, Guangzhou, 510280, Guangdong, China.
Department of Epidemiology, School of Public Health, Southern Medical University, Guangzhou, 510515, Guangdong, China.
Cardiovasc Diabetol. 2025 Apr 2;24(1):153. doi: 10.1186/s12933-025-02711-x.
Cardiovascular diseases (CVD) remain the leading cause of morbidity and mortality globally. Traditional risk models, primarily based on established risk factors, often lack the precision needed to accurately predict new-onset major adverse cardiovascular events (MACE). This study aimed to improve prediction and risk stratification by integrating traditional risk factors with biochemical and metabolomic biomarkers.
We analyzed data from 229,352 participants in the UK Biobank (median age 58.0 years; 45.4% male) who were free of baseline MACE. Biomarker selection was conducted using area under the curve (AUC), minimal joint mutual information maximization (JMIM), and correlation analyses, while Cox proportional hazards models were employed to evaluate the predictive performance of combined traditional risk factors and biomarkers. Optimal binary thresholds were determined utilizing CatBoost and SHAP, leading to the calculation of a Biomarker Risk Score (BRS) for each participant. Multivariable Cox models were conducted to assess the associations of each concerned biomarker and BRS with new-onset endpoints.
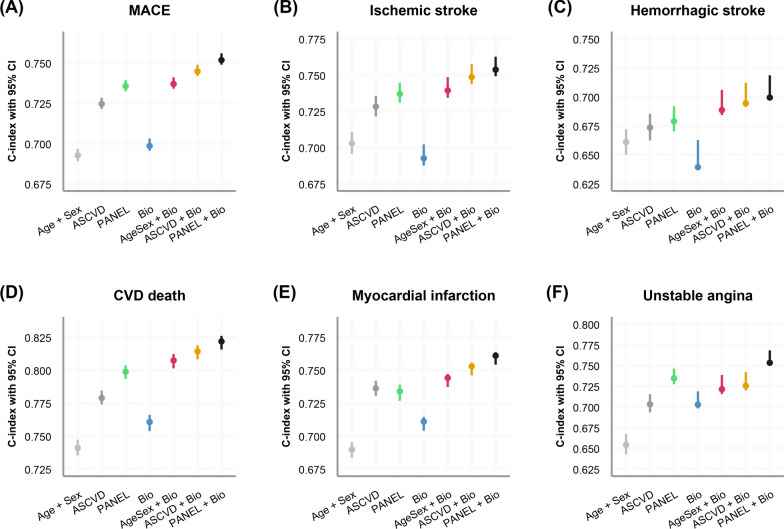
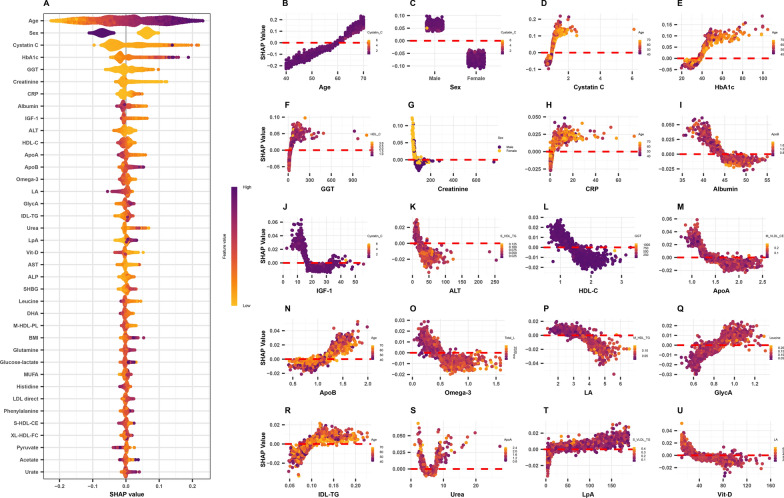
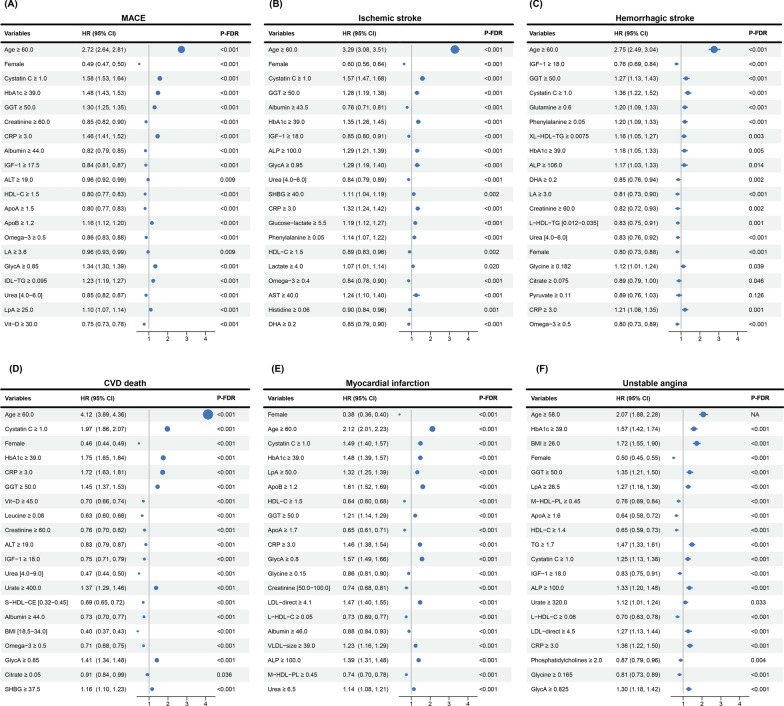
The combination of PANEL + All Biochemistry + Cor0.95 of Nonov Met predictors demonstrated significantly improved discriminative performance compared to traditional models, such as Age + Sex and ASCVD, across all endpoints. Although the prediction for hemorrhagic stroke was suboptimal (C-index = 0.699), C-index values for other outcomes surpassed 0.75, with the highest value (0.822) recorded for CVD-related mortality. Key predictors of new-onset MACE included cystatin C, HbA1c, GlycA, and GGT, while IGF-1 and DHA exhibited potential protective effects. The BRS stratified individuals into low-, intermediate-, and high-risk groups, with the strongest effect observed for CVD death, where the high-risk group had a relative risk of 2.76 (95% CI 2.48-3.07) compared to the low-risk group.
Integrating traditional risk factors and biomarkers improves prediction and risk stratification of new-onset MACE. The BRS shows promise as a tool for identifying high-risk individuals, with the potential to support personalized CVD prevention and management strategies.
心血管疾病(CVD)仍是全球发病和死亡的主要原因。传统风险模型主要基于既定风险因素,往往缺乏准确预测新发主要不良心血管事件(MACE)所需的精度。本研究旨在通过将传统风险因素与生化和代谢组学生物标志物相结合来改善预测和风险分层。
我们分析了英国生物银行中229,352名参与者(中位年龄58.0岁;45.4%为男性)的数据,这些参与者无基线MACE。使用曲线下面积(AUC)、最小联合互信息最大化(JMIM)和相关性分析进行生物标志物选择,同时采用Cox比例风险模型评估传统风险因素与生物标志物组合的预测性能。利用CatBoost和SHAP确定最佳二元阈值,从而为每个参与者计算生物标志物风险评分(BRS)。进行多变量Cox模型以评估每个相关生物标志物和BRS与新发终点的关联。
与传统模型(如年龄+性别和动脉粥样硬化性心血管疾病[ASCVD])相比,PANEL +所有生化指标+非卵巢代谢预测因子的Cor0.95组合在所有终点均显示出显著改善的判别性能。尽管对出血性中风的预测不理想(C指数=0.699),但其他结局的C指数值超过0.75,其中与CVD相关死亡率的C指数值最高(0.822)。新发MACE的关键预测因子包括胱抑素C、糖化血红蛋白(HbA1c)、糖化白蛋白(GlycA)和γ-谷氨酰转移酶(GGT),而胰岛素样生长因子-1(IGF-1)和二十二碳六烯酸(DHA)表现出潜在的保护作用。BRS将个体分为低、中、高风险组,在CVD死亡方面观察到的效应最强,与低风险组相比,高风险组的相对风险为2.76(95%置信区间2.48-3.07)。
整合传统风险因素和生物标志物可改善新发MACE的预测和风险分层。BRS有望作为识别高风险个体的工具,有可能支持个性化的CVD预防和管理策略。