Tavornshevin Pipu, Chantranuwatana Poonchavist, Thanthitaweewat Vorawut, Wongsrichanalai Virissorn, Sriprasart Thitiwat, Leelayuwatanakul Nophol
Division of Pulmonary and Critical Care Medicine, Department of Medicine, Chulalongkorn University, Bangkok, Thailand.
Department of Pathology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand.
Tuberc Respir Dis (Seoul). 2025 Jul;88(3):545-556. doi: 10.4046/trd.2024.0134. Epub 2025 Apr 3.
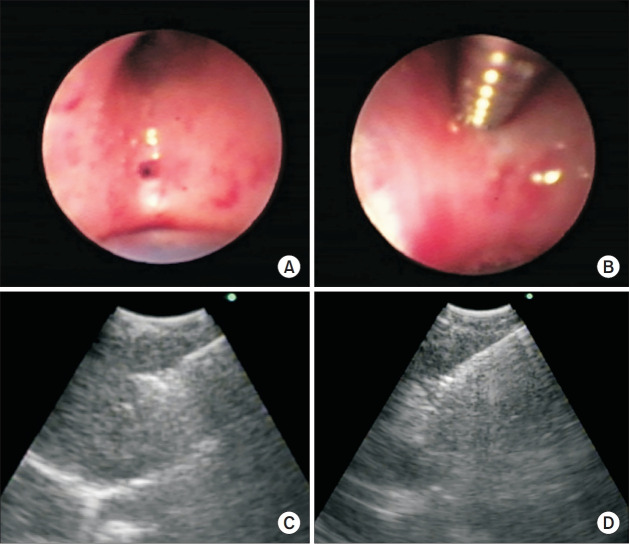
Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is a predominantly used method for lymph node (LN) metastasis assessment. This study aims to identify tissue adequacy improvement with the addition of EBUS-guided miniforcep biopsy (EBUS-MFB) to EBUS-TBNA in sampling LNs.
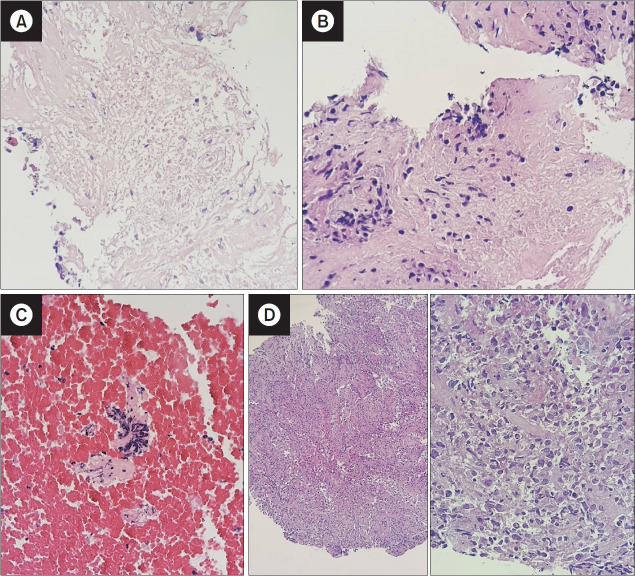
We assessed tissue adequacy in patients with mediastinal and hilar lymphadenopathy, comparing the combination of EBUS-MFB and EBUS-TBNA with EBUS-TBNA alone. EBUS-MFB was performed with the guide sheath (GS) dilatation technique. Tissue adequacy was a tumor cell count (TCC) of >100 and neoplastic cell neoplastic cell estimate of >25%. Further, we reported the diagnostic yield, tumor cell characteristics, and safety outcomes.
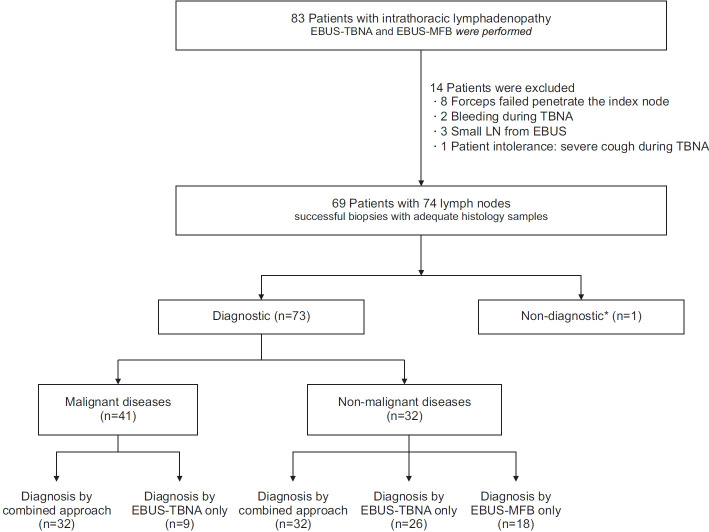
Among 69 patients (74 nodes), malignant diseases were diagnosed in 41 nodes using both techniques. Tissue adequacy with EBUS-TBNA (93.8% in 30/32 nodes) was comparable with the combined group (96.9% in 31/32 nodes, p=0.317). EBUS-TBNA yielded higher TCC (84.4% with >1,000 cells) than EBUS-MFB (53.1%, p=0.004). The combined approach significantly improved the diagnostic yield in non-malignant diseases compared with EBUS-TBNA alone (97% vs. 78.8%, p=0.014). Of the 32 nodes, 20 demonstrated discordant results between EBUS-TBNA and EBUS-MFB, with EBUS-MFB correctly diagnosing six nodes that EBUS-TBNA misdiagnosed. The complication rate was low (2.9%) with only minor bleeding reported.
EBUS-TBNA alone and the combination of EBUS-MFB and EBUS-TBNA demonstrated comparable tissue adequacy, with EBUS-TBNA exhibiting better specimen characteristics, potentially sufficient for various molecular analyses. The addition of EBUS-MFB, performed using the GS-dilatation technique, to EBUS-TBNA improved the diagnostic yield and proved to be a safe and efficient approach, particularly in non-malignant diseases.
支气管内超声引导下经支气管针吸活检术(EBUS-TBNA)是评估淋巴结(LN)转移的主要方法。本研究旨在确定在EBUS-TBNA基础上增加EBUS引导下微型钳活检术(EBUS-MFB)对LN采样时组织充足性的改善情况。
我们评估了纵隔和肺门淋巴结肿大患者的组织充足性,将EBUS-MFB与EBUS-TBNA联合使用的情况与单独使用EBUS-TBNA的情况进行了比较。EBUS-MFB采用导鞘(GS)扩张技术进行。组织充足性定义为肿瘤细胞计数(TCC)>100且肿瘤细胞估计数>25%。此外,我们报告了诊断率、肿瘤细胞特征和安全性结果。
在6个患者(74个淋巴结)中,两种技术共诊断出41个淋巴结为恶性疾病。EBUS-TBNA的组织充足性(30/32个淋巴结中为93.8%)与联合组(31/32个淋巴结中为96.9%,p=0.317)相当。EBUS-TBNA产生的TCC高于EBUS-MFB(>1000个细胞的占84.4%对53.1%,p=0.004)。与单独使用EBUS-TBNA相比,联合方法显著提高了非恶性疾病的诊断率(97%对78.8%,p=0.014)。在32个淋巴结中,20个在EBUS-TBNA和EBUS-MFB之间显示出不一致的结果,EBUS-MFB正确诊断了EBUS-TBNA误诊的6个淋巴结。并发症发生率较低(2.9%),仅报告有轻微出血。
单独使用EBUS-TBNA以及EBUS-MFB与EBUS-TBNA联合使用显示出相当可比的组织充足性,EBUS-TBNA表现出更好的标本特征,可能足以进行各种分子分析。在EBUS-TBNA基础上增加采用GS扩张技术进行的EBUS-MFB提高了诊断率,并且被证明是一种安全有效的方法,特别是在非恶性疾病中。