Serre Justine, Mulier Guillaume, Boud'hors Charlotte, Lemerle Marie, Abdel-Nabey Moustafa, Orvain Corentin, Chaba Anis, Biard Lucie, Demiselle Julien, Zafrani Lara
Department of Medical Intensive Care, Hôpital Saint-Louis, AP-HP, Paris, France.
Department of Biostatistics and Medical Information, AP-HP, Hôpital Saint-Louis, Université Paris Cité, Paris, France.
Ann Intensive Care. 2025 Apr 4;15(1):49. doi: 10.1186/s13613-025-01439-x.
In the context of tumor lysis syndrome (TLS), the optimal timing and criteria for initiating kidney replacement therapy (KRT) remain unclear. This study aims to assess the effect of initiating KRT at various phosphatemia thresholds on Major Adverse Kidney Events at day 30 (MAKE30).
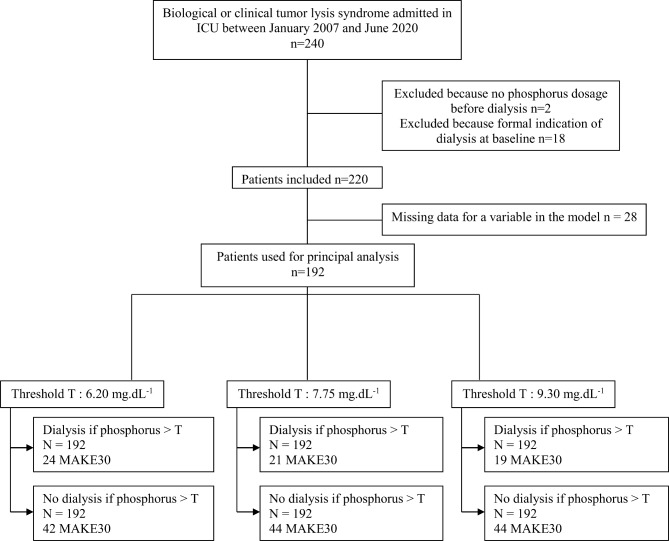
We retrospectively emulated a pragmatic clinical trial comparing the effect of KRT initiation at various phosphatemia thresholds versus a conventional approach during TLS on MAKE30. All consecutive patients admitted to the ICU at Saint-Louis University hospital in Paris and Angers University hospital between January 2007 and June 2020, presenting with laboratory TLS were included. The design criteria of a clinical trial were mimicked by using the cloning, censoring and weighting method. The primary outcome was the MAKE30 composite outcome, considering only KRT requirement between day 7 and day 30 for the dialysis criteria. We evaluated multiple phosphatemia thresholds to guide KRT initiation, ranging from 6.20 mg.dL to 9.30 mg.dL. Among the initial population of 220 patients, 192 were included in the emulated trial (median age 60 years old, with non-Hodgkin Lymphoma and Acute Leukemia being the most frequent hematological malignancies). TLS-related AKI occurred in 140 patients, and 75 patients met the criteria for MAKE30. Regardless of the phosphate threshold considered, KRT initiation based on phosphate level was not associated with a significant difference in the MAKE30 rate. KRT requirement during the first 7 days (Odd Ratio [OR] 4.01 [1.65-4.86], p = 0.003) and non-renal SOFA (OR 1.39 per 1 point increment [1.25-1.57], p < 0.001) were identified as factors associated with MAKE30 (multivariable analysis).
Our results do not support the strategy of KRT initiation based on a sole critical phosphatemia level in TLS patients.
在肿瘤溶解综合征(TLS)的背景下,启动肾脏替代治疗(KRT)的最佳时机和标准仍不明确。本研究旨在评估在不同血磷阈值下启动KRT对第30天严重不良肾脏事件(MAKE30)的影响。
我们回顾性模拟了一项实用的临床试验,比较在TLS期间不同血磷阈值下启动KRT与传统方法对MAKE30的影响。纳入2007年1月至2020年6月期间在巴黎圣路易大学医院和昂热大学医院重症监护病房住院的所有连续出现实验室确诊TLS的患者。采用克隆、删失和加权方法模拟临床试验的设计标准。主要结局是MAKE30复合结局,仅将第7天至第30天的KRT需求纳入透析标准。我们评估了多个血磷阈值以指导KRT启动,范围从6.20mg/dL至9.30mg/dL。在最初的220例患者中,192例被纳入模拟试验(中位年龄60岁,非霍奇金淋巴瘤和急性白血病是最常见的血液系统恶性肿瘤)。140例患者发生了TLS相关急性肾损伤,75例患者符合MAKE30标准。无论考虑何种血磷阈值,基于血磷水平启动KRT与MAKE30发生率的显著差异无关。第1个7天内的KRT需求(比值比[OR]4.01[1.65 - 4.86],p = 0.003)和非肾性序贯器官衰竭评估(SOFA)评分(每增加1分OR为1.39[1.25 - 1.57],p < 0.001)被确定为与MAKE30相关的因素(多变量分析)。
我们的结果不支持在TLS患者中基于单一临界血磷水平启动KRT的策略。