Malacatus-Arboleda Aurora, Barbotó-Ramírez Erick, Sánchez Gonzalo E, Moscoso Bernard, Rhodes Lauren A, Coloma Josefina, Guevara Ángel, Espinoza-Fuentes Fernando, Fernández-Cadena Juan Carlos, Morey-León Gabriel, Andrade-Molina Derly
Laboratorio de Ciencias Ómicas, Facultad de Ciencias de la Salud, Universidad Espíritu Santo, Samborondón, Ecuador.
Facultad de Ciencias Sociales y Humanísticas, Centro de Investigaciones Económicas, Escuela Superior Politécnica del Litoral, ESPOL, Guayaquil, Ecuador.
Front Public Health. 2025 Mar 25;13:1537049. doi: 10.3389/fpubh.2025.1537049. eCollection 2025.
Timely distribution of COVID-19 vaccines was particularly important for developing countries that do not have strong health systems and related infrastructure. We analyze data from the Guayas province of Ecuador, an area particularly affected by the pandemic, to determine the seroprevalence of SARS-CoV-2 and the effect of the timing of the second dose of COVID-19 vaccines on the seroprevalence SARS-CoV-2 IgG antibodies.
This cross-sectional study involved 1,761 individuals aged 18 and older who voluntarily enrolled prior to and during the initial phase of vaccine rollout in Ecuador (October 2020 to July 2022). IgG anti-SARS-CoV-2 RBD antibodies were assessed by an ELISA to evaluate the immune response to Pfizer (BioNTech, Spike mRNA) and AstraZeneca (Oxford, AstraZeneca Spike) vaccine in the Guayas province. Ordinary least squares (OLS) regressions were employed to determine the effect of delayed second doses later than prescribed by the manufacturer for both vaccines.
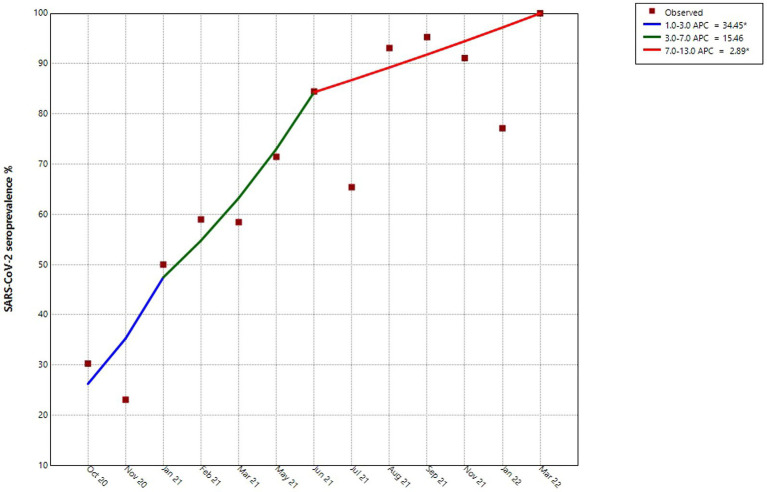
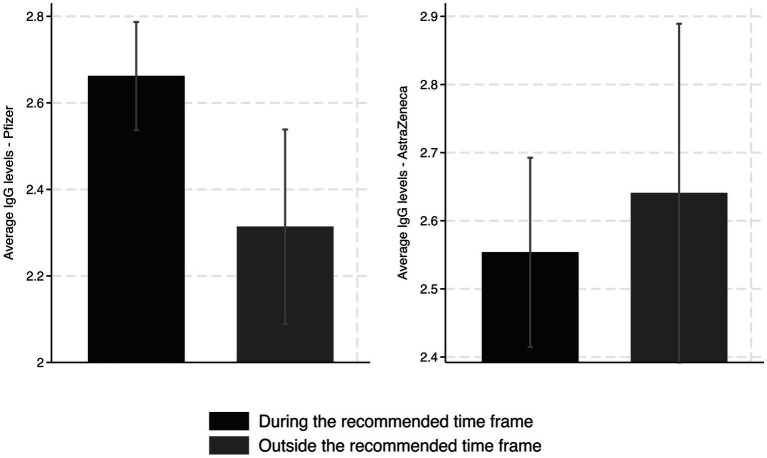
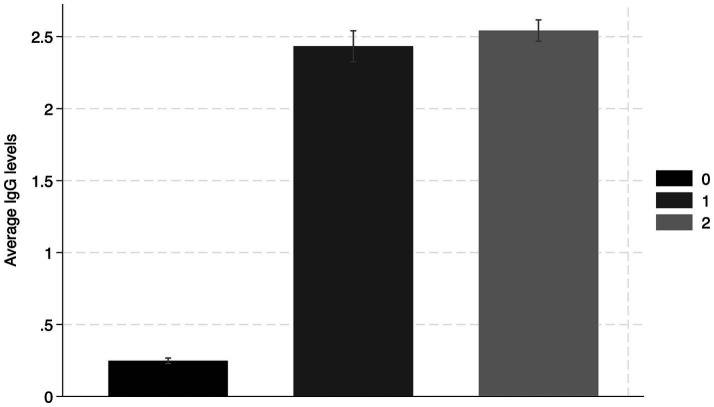
Before the vaccination campaign, we estimated an RBD IgG seroprevalence of 27.7% (95% CI: 23.6-27, = 469). The estimate increased to 89.4% (95% CI: 87.7-91.18, = 1,235) after the first vaccine dose and to 92.6% (95% CI: 90.7-94.5, = 748) after the second dose. Individuals who received the second dose of the Pfizer vaccine later than the recommended dose showed significantly lower levels of IgG antibodies 2-3 weeks after receiving the second dose than those who received the dose within the recommended timeframe. Furthermore, we did not find any effect on RBD IgG antibody levels in those who received a second dose of the AstraZeneca vaccine during the first and second parts of the recommended vaccination window.
The results suggest that a significant portion of the study population was already infected with SARS-CoV-2 prior to the vaccination. As expected, seropositivity increased alongside vaccination efforts. We determined that Pfizer vaccine recipients should be adhered to vaccine timing guidelines. Furthermore, resource-limited countries should consider administering vaccines with flexibility in dosing intervals, such as AstraZeneca, as it allows for a wider time frame without significantly reducing the boosting of IgG antibodies.
对于卫生系统和相关基础设施薄弱的发展中国家而言,及时分发新冠疫苗尤为重要。我们分析了厄瓜多尔瓜亚斯省的数据,该地区受疫情影响尤为严重,以确定新冠病毒的血清阳性率以及第二剂新冠疫苗接种时间对新冠病毒IgG抗体血清阳性率的影响。
这项横断面研究涉及1761名18岁及以上的个体,他们在厄瓜多尔疫苗推广的初始阶段之前及期间(2020年10月至2022年7月)自愿报名参加。通过酶联免疫吸附测定法评估抗新冠病毒受体结合域IgG抗体,以评估瓜亚斯省对辉瑞(BioNTech,刺突mRNA)和阿斯利康(牛津,阿斯利康刺突)疫苗的免疫反应。采用普通最小二乘法回归来确定两种疫苗第二剂延迟接种超过制造商规定时间的影响。
在疫苗接种运动之前,我们估计受体结合域IgG血清阳性率为27.7%(95%置信区间:23.6 - 27,n = 469)。在接种第一剂疫苗后,该估计值增至89.4%(95%置信区间:87.7 - 91.18,n = 1235),在接种第二剂疫苗后增至92.6%(95%置信区间:90.7 - 94.5,n = 748)。辉瑞疫苗第二剂接种时间晚于推荐剂量的个体,在接种第二剂疫苗2至3周后,其IgG抗体水平显著低于在推荐时间范围内接种的个体。此外,我们未发现那些在推荐接种窗口的第一部分和第二部分期间接种阿斯利康疫苗第二剂的个体,其受体结合域IgG抗体水平受到任何影响。
结果表明,在接种疫苗之前,很大一部分研究人群已感染新冠病毒。正如预期的那样,血清阳性率随着疫苗接种工作而上升。我们确定辉瑞疫苗接种者应遵循疫苗接种时间指南。此外,资源有限的国家应考虑灵活安排疫苗接种间隔,如阿斯利康疫苗,因为它允许更宽的时间范围,且不会显著降低IgG抗体的增强效果。