Csipor Fodor Alpár, Huțanu Dragoș, Budin Corina Eugenia, Ianoși Maria Beatrice, Rachiș Delia Liana, Sárközi Hédi-Katalin, Vultur Mara Andreea, Jimborean Gabriela
Pulmonology Department, County Emergency Hospital Miercurea-Ciuc, 530173 Miercurea-Ciuc, Romania.
Pulmonology Department, "George Emil Palade" University of Medicine, Pharmacy, Science and Technology of Târgu Mureș, 540139 Târgu Mureș, Romania.
J Clin Med. 2025 Mar 29;14(7):2369. doi: 10.3390/jcm14072369.
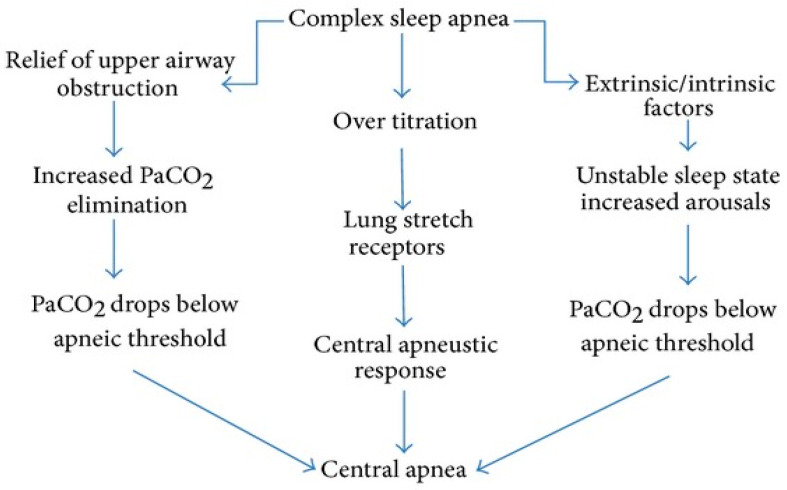
Central sleep apnea (CSA) is a heterogeneous group of sleep-related breathing disorders characterized by intermittent absence of respiratory effort during sleep. CSA results from impaired neurological signaling from the respiratory centers to the respiratory muscles, leading to airflow cessation for at least 10 s. Major causes include heart failure, opioid use, central neurological disorders, and altitude exposure. This review outlines the pathophysiology of CSA, emphasizing ventilatory instability and brainstem dysfunction as key mechanisms. It details the classification of CSA subtypes, including Cheyne-Stokes respiration, high-altitude CSA, and drug-induced CSA. Clinical manifestations range from excessive daytime sleepiness to cardiovascular complications. Diagnostic approaches encompass polygraphy, polysomnography, and various laboratory tests to evaluate comorbidities. Treatment requires a multidisciplinary approach, addressing underlying conditions while utilizing positive airway pressure (PAP) therapy, adaptive servo-ventilation (ASV), supplemental oxygen, and pharmacological interventions. Newer modalities, such as phrenic nerve stimulation, offer promising outcomes for CSA management. This review underscores the necessity of an individualized, interdisciplinary strategy to improve patient outcomes in CSA.
中枢性睡眠呼吸暂停(CSA)是一组与睡眠相关的呼吸障碍的异质性疾病,其特征是睡眠期间呼吸努力间歇性缺失。CSA是由于呼吸中枢向呼吸肌的神经信号传递受损,导致气流停止至少10秒。主要病因包括心力衰竭、阿片类药物使用、中枢神经系统疾病和高原暴露。本综述概述了CSA的病理生理学,强调通气不稳定和脑干功能障碍是关键机制。它详细介绍了CSA亚型的分类,包括潮式呼吸、高原性CSA和药物性CSA。临床表现从白天过度嗜睡到心血管并发症不等。诊断方法包括多导睡眠图、多导睡眠监测以及各种实验室检查以评估合并症。治疗需要多学科方法,在利用气道正压通气(PAP)治疗、适应性伺服通气(ASV)、补充氧气和药物干预的同时解决潜在疾病。较新的治疗方式,如膈神经刺激,为CSA的管理提供了有前景的结果。本综述强调了采取个体化、跨学科策略以改善CSA患者预后的必要性。