Ali Abdelrahman, Koutroumpakis Efstratios, Song Juhee, Booser Daniel, Barcenas Carlos H, Tripathy Debu, Barac Ana, Palaskas Nicolas L, Deswal Anita
Department of Cardiology, University of Texas MD Anderson Cancer Center, Houston, Texas, USA. Electronic address: https://twitter.com/Abdelcards.
Department of Cardiology, University of Texas MD Anderson Cancer Center, Houston, Texas, USA. Electronic address: https://twitter.com/EKoutroumpakis.
JACC CardioOncol. 2025 Apr;7(3):203-215. doi: 10.1016/j.jaccao.2024.12.007. Epub 2025 Feb 25.
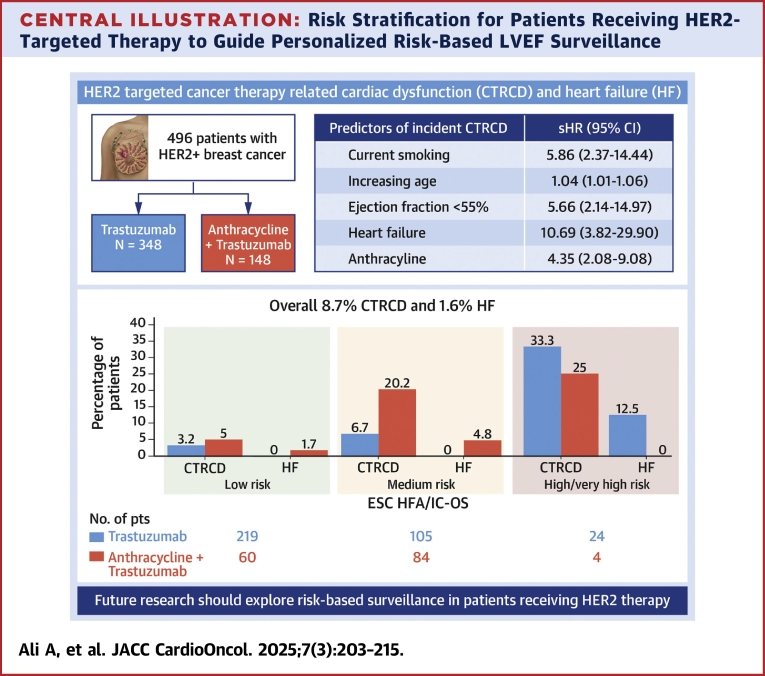
Although patient factors and sequential anthracycline use contribute to risk for cancer therapy-related cardiac dysfunction (CTRCD) with HER2-directed cancer therapy, frequent (every 3 months) left ventricular ejection fraction (LVEF) surveillance is recommended irrespective of baseline risk.
The aim of this study was to examine the incidence of trastuzumab-associated CTRCD in a contemporary cohort with HER2-positive breast cancer and assess the performance of a risk assessment tool to identify patients at low risk for CTRCD to guide risk-based surveillance strategies.
A retrospective cohort of patients with HER2-positive breast cancer treated with trastuzumab at a tertiary cancer center was examined. Patients were categorized as low, medium, and high or very high risk for CTRCD by Heart Failure Association/International Cardio-Oncology Society risk assessment.
Of 496 patients treated with trastuzumab, 29.8% also received anthracyclines. Over a median follow-up period of 51 months, 8.7% developed CTRCD, but only 1.6% had associated heart failure (HF). CTRCD rates were 3.6%, 12.8%, and 32.1% in low-risk, medium-risk, and high or very high risk groups, respectively. HF incidence was 0.4% in the low-risk group and 2.1% in the medium-risk group, with no HF in patients at low- or medium-risk who received trastuzumab without anthracyclines. HF was observed in 11% of high-risk patients. The risk assessment had a negative predictive value for CTRCD in low vs moderate- or high-risk patients of 96.4% (95% CI: 93.5%-98.3%).
The findings support the exploration of a prospective personalized risk-based approach to cardiac LVEF surveillance during trastuzumab therapy. Less frequent LVEF monitoring in low-risk patients may optimize resource use and reduce patient burden without compromising safety.
尽管患者因素和序贯使用蒽环类药物会增加HER2靶向癌症治疗相关的心脏功能障碍(CTRCD)风险,但无论基线风险如何,均建议频繁(每3个月)监测左心室射血分数(LVEF)。
本研究旨在调查当代HER2阳性乳腺癌队列中曲妥珠单抗相关CTRCD的发生率,并评估一种风险评估工具在识别CTRCD低风险患者以指导基于风险的监测策略方面的性能。
对一家三级癌症中心接受曲妥珠单抗治疗的HER2阳性乳腺癌患者进行回顾性队列研究。根据心力衰竭协会/国际心脏肿瘤学会风险评估,将患者分为CTRCD低、中、高或极高风险组。
在496例接受曲妥珠单抗治疗的患者中,29.8%还接受了蒽环类药物治疗。在中位随访期51个月内,8.7%的患者发生了CTRCD,但只有1.6%的患者出现了相关心力衰竭(HF)。低风险、中风险和高或极高风险组的CTRCD发生率分别为3.6%、12.8%和32.1%。低风险组的HF发生率为0.4%,中风险组为2.1%,未接受蒽环类药物的低风险或中风险患者未发生HF。高风险患者中有11%出现HF。在低风险与中高风险患者中,风险评估对CTRCD的阴性预测值为96.4%(95%CI:93.5%-98.3%)。
这些发现支持在曲妥珠单抗治疗期间探索一种前瞻性的基于个体风险的心脏LVEF监测方法。对低风险患者减少LVEF监测频率可能会优化资源利用并减轻患者负担,同时不影响安全性。