Sardesai Sagar, Sukumar Jasmine, Kassem Mahmoud, Palettas Marilly, Stephens Julie, Morgan Evan, Addison Daniel, Baliga Ragavendra, Stover Daniel G, VanDeusen Jeffrey, Williams Nicole, Cherian Mathew, Lustberg Maryam, Wesolowski Robert, Ramaswamy Bhuvaneswari
Stefanie Spielman Comprehensive Breast Cancer, The Ohio State University, Columbus, OH, 43210, USA.
Division of Medical Oncology, Comprehensive Cancer Center, The Ohio State University Wexner Medical Center, 1204A Lincoln Tower, 1800 Cannon Dr, Columbus, OH, USA.
Cardiooncology. 2020 Nov 5;6(1):26. doi: 10.1186/s40959-020-00081-9.
Trastuzumab-induced cardiotoxicity (TIC) can lead to early discontinuation of adjuvant therapy, however there is limited evidence on long-term survival outcomes in patients with operable human epidermal growth factor receptor 2 (HER2)-positive breast cancer (BC) experiencing treatment interruption or discontinuation.
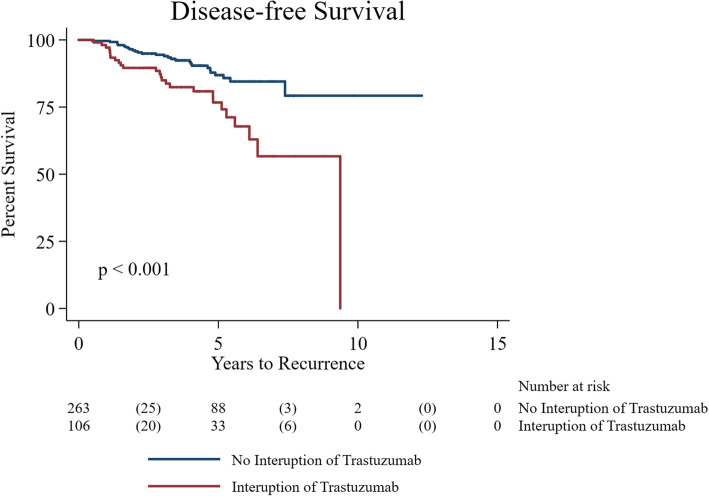
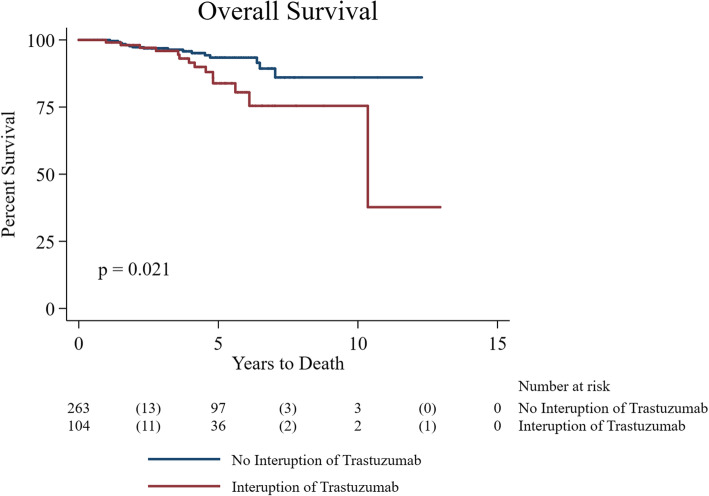
The primary objective of the study was to evaluate disease-free survival (DFS) in non-metastatic, HER2-positive, female BC patients who experienced treatment interruption or early discontinuation of trastuzumab therapy. Clinical and histopathological data were collected on 400 patients at The Ohio State University, an NCI-designated comprehensive cancer center between January 2005 and December 2015. Treatment interruption was defined as any delay of ≥2 weeks during trastuzumab therapy, including permanent cessation prior to completing planned therapy. TIC was defined as LVEF < 50% or > 15 points decline from baseline as evaluated by 2D echocardiogram after initiation of (neo) adjuvant therapy. DFS was defined as the time from diagnosis to first recurrence (loco-regional or distant recurrence) including second primary BC or death. Overall survival (OS) was defined as the time from diagnosis to death or last known follow up. OS/DFS estimates were generated using Kaplan-Meier methods and compared using Log-rank tests. Cox proportional hazard models were used to calculate adjusted hazard ratios (aHR) for OS/DFS.
A total of 369 patients received trastuzumab therapy; 106 (29%) patients experienced treatment interruption at least once and 42 (11%) permanently discontinued trastuzumab prior to completing planned therapy. TIC was the most common reason for interruption (66 patients, 62%). The median duration of trastuzumab in patients with treatment interruption was 11.3 months (range: 0.5-16.9) with 24 (23%) patients receiving ≤6 months of therapy. This duration includes the time delay related to treatment interruption. Patients with any treatment interruption had worse DFS (aHR: 4.4, p = 0.001) and OS (aHR: 4.8, p < 0.001) after adjusting for age, stage, grade, ER, node status and TIC.
Treatment interruption or early discontinuation of trastuzumab therapy in early HER2-positive BC, most often from TIC, is an independent prognostic marker for worse DFS and OS in operable HER2-positive BC. Future prospective studies should consider targeting at-risk populations and optimizing cardiac function to avoid interruption in trastuzumab therapy.
曲妥珠单抗诱导的心脏毒性(TIC)可导致辅助治疗提前中断,然而,对于可手术的人表皮生长因子受体2(HER2)阳性乳腺癌(BC)患者,在治疗中断或终止后长期生存结局的证据有限。
本研究的主要目的是评估经历曲妥珠单抗治疗中断或提前终止的非转移性、HER2阳性女性BC患者的无病生存期(DFS)。2005年1月至2015年12月期间,在国立癌症研究所指定的综合癌症中心俄亥俄州立大学收集了400例患者的临床和组织病理学数据。治疗中断定义为曲妥珠单抗治疗期间任何≥2周的延迟,包括在完成计划治疗前永久停药。TIC定义为在(新)辅助治疗开始后通过二维超声心动图评估的左心室射血分数(LVEF)<50%或较基线下降>15个百分点。DFS定义为从诊断到首次复发(局部区域或远处复发)的时间,包括第二原发性BC或死亡。总生存期(OS)定义为从诊断到死亡或最后一次已知随访的时间。使用Kaplan-Meier方法生成OS/DFS估计值,并使用对数秩检验进行比较。使用Cox比例风险模型计算OS/DFS的调整风险比(aHR)。
共有369例患者接受曲妥珠单抗治疗;106例(29%)患者至少经历过一次治疗中断,42例(11%)在完成计划治疗前永久停用曲妥珠单抗。TIC是中断治疗的最常见原因(66例患者,62%)。治疗中断患者的曲妥珠单抗中位治疗持续时间为11.3个月(范围:0.5-16.9),24例(23%)患者接受治疗≤6个月。该持续时间包括与治疗中断相关的时间延迟。在调整年龄、分期、分级、雌激素受体、淋巴结状态和TIC后,任何治疗中断的患者DFS(aHR:4.4,p=0.001)和OS(aHR:4.8,p<0.001)更差。
早期HER2阳性BC患者曲妥珠单抗治疗的中断或提前终止,最常见的原因是TIC,是可手术HER2阳性BC患者DFS和OS较差的独立预后标志物。未来的前瞻性研究应考虑针对高危人群并优化心脏功能,以避免曲妥珠单抗治疗中断。