García-Rodríguez Paula, Lamana-Vallverdú Marcel, Guamán-Pilco Daisy R, Penalba Anna, Ramiro Laura, Simats Alba, Faura Júlia, Bustamante Alejandro, Díaz-Troyano Noelia, Montaner Joan
Neurovascular Research Laboratory, Vall d'Hebron Institute of Research (VHIR) Universitat Autònoma de Barcelona Barcelona Spain.
Cerebrovascular Research Laboratory, Instituto de Investigaciones Biomédicas de Barcelona (IIBB) Consejo Superior de Investigaciones Científicas (CSIC) Barcelona Spain.
J Am Heart Assoc. 2025 May 6;14(9):e036727. doi: 10.1161/JAHA.124.036727. Epub 2025 Apr 17.
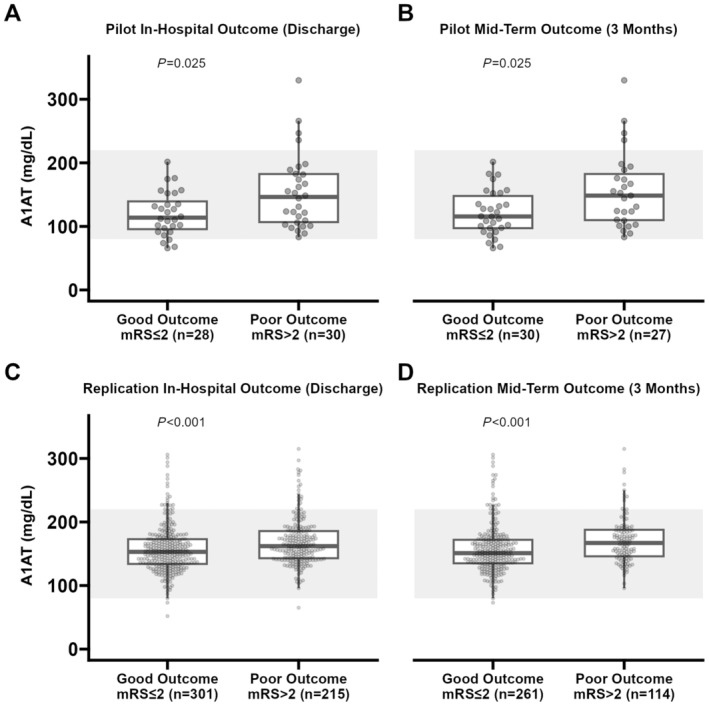
This study aimed to investigate whether A1AT (α-1 antitrypsin) bloodstream levels, measured acutely after ischemic stroke, can predict the outcome of patients with stroke.
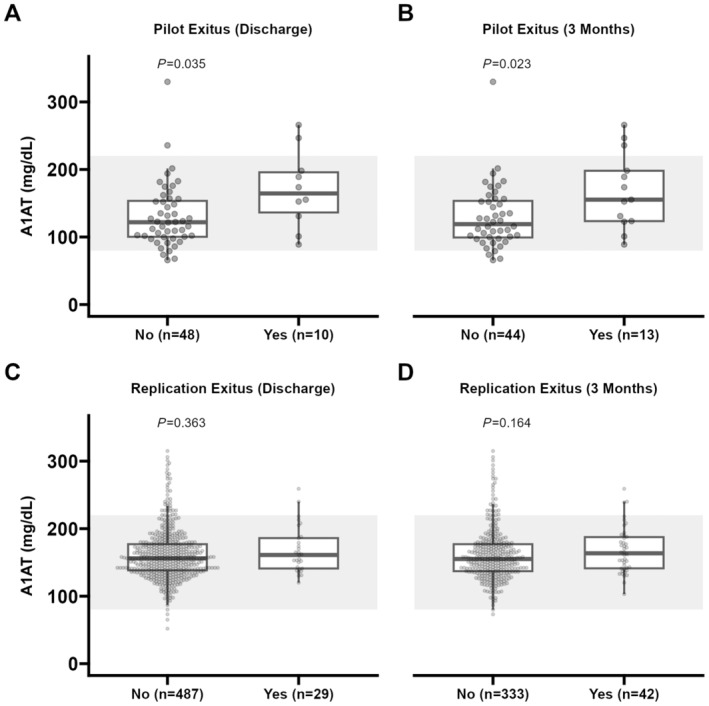
Two cohorts of patients with stroke were studied independently and retrospectively: a pilot cohort of 59 patients and a larger replicative study with 527 patients. Blood samples were drawn at hospital admission (<6 hours after stroke onset) before any treatment was given. A1AT levels were analyzed. Patients were followed after the event, and functional outcomes were evaluated at in-hospital (discharge) and midterm (third month) follow-up according to the modified Rankin Scale (considering modified Rankin Scale score >2 a poor outcome). Association studies between A1AT levels and functional outcomes were conducted. We also evaluated the added value of A1AT as a prognostic biomarker over the clinical model (sex, age, premorbid modified Rankin Scale and National Institutes of Health Stroke Scale scores) with the likelihood ratio test. In both studies, the levels of A1AT were higher in patients who had worse outcomes, were older, and had higher National Institutes of Health Stroke Scale scores at admission. In the pilot study, higher levels of A1AT were also associated with death at discharge and at 3 months after stroke (=0.035 and =0.023, respectively). The addition of A1AT to the clinical model did not show enough evidence of increasing the fit of the model to the data in either cohort.
Based on our data, we cannot claim that A1AT is an independent biomarker of ischemic stroke. Nevertheless, A1AT is potentially involved in stroke outcomes and might be explored as a potential therapeutic target.
本研究旨在调查缺血性卒中后急性测量的A1AT(α-1抗胰蛋白酶)血流水平是否可预测卒中患者的预后。
对两组卒中患者进行了独立的回顾性研究:一个由59名患者组成的试点队列和一个有527名患者的更大规模的重复研究。在给予任何治疗前,于入院时(卒中发作后<6小时)采集血样。分析A1AT水平。事件发生后对患者进行随访,并根据改良Rankin量表在住院(出院时)和中期(第三个月)随访时评估功能结局(将改良Rankin量表评分>2视为不良结局)。进行了A1AT水平与功能结局之间的关联研究。我们还通过似然比检验评估了A1AT作为预后生物标志物相对于临床模型(性别、年龄、病前改良Rankin量表和美国国立卫生研究院卒中量表评分)的附加值。在两项研究中,结局较差、年龄较大且入院时美国国立卫生研究院卒中量表评分较高的患者A1AT水平较高。在试点研究中,较高的A1AT水平还与出院时及卒中后3个月的死亡相关(分别为=0.035和=0.023)。在任一队列中,将A1AT添加到临床模型中均未显示出足够证据表明该模型对数据的拟合度有所提高。
基于我们的数据,我们不能声称A1AT是缺血性卒中的独立生物标志物。尽管如此,A1AT可能参与卒中结局,可作为潜在治疗靶点进行探索。