Ronald Kato, Ronald Kantu, Ambaru Jacinta, Sekiwunga Dan
Gulu University Faculty of Medicine, Kampala Uganda Gulu Uganda.
Department of Internal Medicine, Faculty of Health Sciences Makerere University Kampala Uganda.
Clin Case Rep. 2025 Apr 21;13(4):e70469. doi: 10.1002/ccr3.70469. eCollection 2025 Apr.
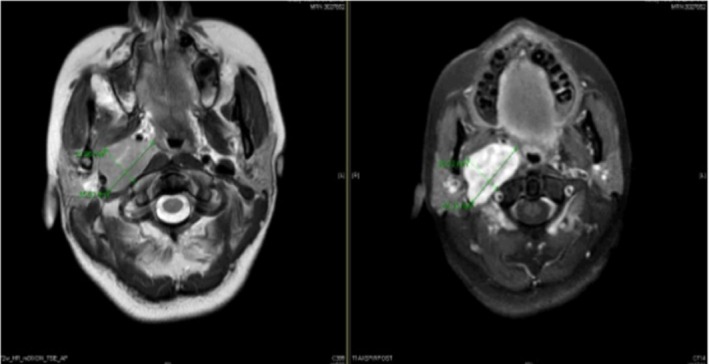
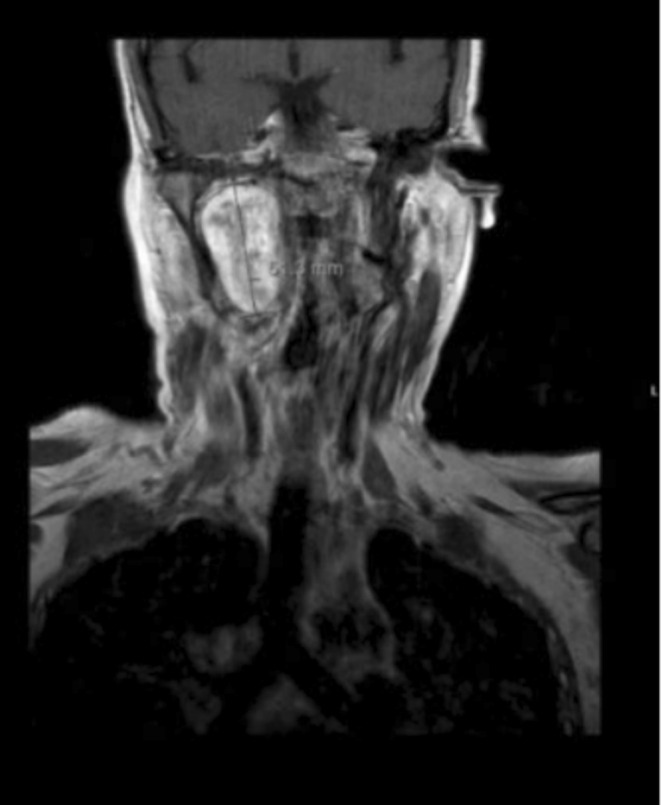
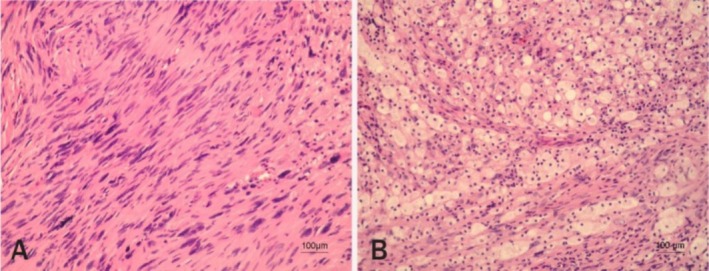
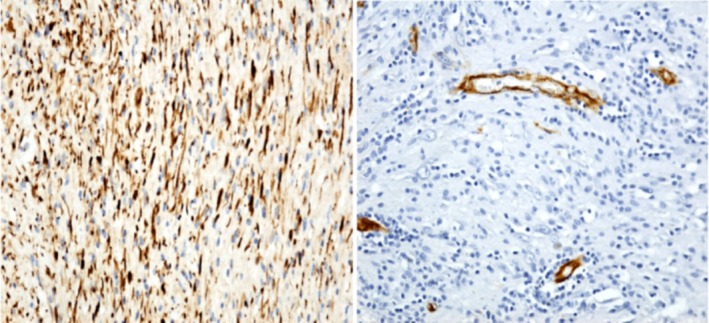
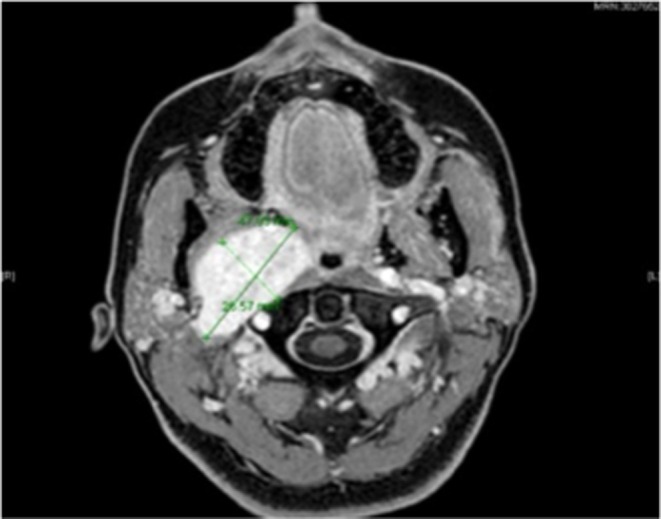
Vagus schwannomas are rare, benign masses that arise in the cervical region but can develop anywhere along the Vagus nerve. In most cases, patients present in their third to sixth decades, with neck swelling and hoarseness; herein, we discuss a case report of a 41-year-old female who presented with slurred speech and locking of her tongue and was diagnosed with Vagus schwannoma. The patient had an inability to speak properly and locking of her tongue during speech, with pain to the right side of the neck as Intermittent, prompted by turning her head to the right and shooting pain to her shoulder, which is short-lived, with a sensation of difficulty swallowing and talking that is alleviated by moving her head to a neutral position. On examination, there was mild neck stiffness, fasciculations of the tongue, and left deviation of the tongue with inability to swallow. Blood pressure was 128/70 mmHg with 42 bpm bradycardia, which was persistent on several readings, with a small right neck mass measuring 1 cm × 2 cm, non-tender on palpation. Imaging studies showed a well-defined ovoid lesion centered in the right retrostyloid parapharyngeal space measuring 3.3 × 2.1 × 3.8 cm with central T2 hyperintensities representing a nerve sheath tumor that appears stable in size and morphology. The histology report typically displayed a characteristic pattern with two distinct tissue types, Antoni A and Antoni B, with tightly packed spindle cells arranged in palisades around a central verocay body and a looser arrangement of myxoid matrix. Immunohistochemistry showed lesional cells had strong immunopositivity for S100 and were negative for CD34. Hence, the conclusion of a Vagus nerve schwannoma. Patient was sent to the radiation oncology team and was started on Cyberknife 25 Gy treatment in five fractions, which were completed and sent for re-evaluation and follow-up. There was no surgical intervention in this case due to the delicate anatomical location of the mass; hence, Cyberknife radiation was the best option for treatment. Vagus schwannomas are rare, benign masses that usually develop in the cervical region but can arise anywhere along the Vagus nerve. Patients may be asymptomatic, but in most cases, they present in their third to sixth decades; hence, they should be considered in patients with otherwise unexplained bradycardia, with a history of dysphagia, slurred speech, and cervical masses.
迷走神经鞘瘤是一种罕见的良性肿块,起源于颈部区域,但可沿迷走神经的任何部位发生。在大多数情况下,患者在30至60岁出现症状,表现为颈部肿胀和声音嘶哑;在此,我们讨论一例41岁女性病例报告,该患者出现言语不清和舌头卡顿,被诊断为迷走神经鞘瘤。患者说话时无法正常发音且舌头卡顿,颈部右侧间歇性疼痛,向右侧转头时诱发,疼痛放射至肩部,持续时间短,伴有吞咽和说话困难的感觉,将头部恢复到中立位置可缓解。检查发现有轻度颈部僵硬、舌肌束颤,舌头向左偏斜且无法吞咽。血压为128/70 mmHg,心率42次/分,心动过缓,多次测量均持续存在,右侧颈部有一个1 cm×2 cm的小肿块,触诊无压痛。影像学检查显示,在右侧茎突后咽旁间隙有一个边界清晰的椭圆形病变,大小为3.3×2.1×3.8 cm,中央T2高信号,提示为神经鞘瘤,其大小和形态稳定。组织学报告通常显示出一种特征性模式,有两种不同的组织类型,即Antoni A和Antoni B,紧密排列的梭形细胞围绕中央Verocay小体呈栅栏状排列,黏液样基质排列较疏松。免疫组化显示病变细胞对S100呈强免疫阳性,对CD34呈阴性。因此,诊断为迷走神经鞘瘤。患者被转至放射肿瘤学团队,开始接受射波刀25 Gy分五次治疗,治疗完成后进行重新评估和随访。由于肿块的解剖位置精细,该病例未进行手术干预;因此,射波刀放射治疗是最佳治疗选择。迷走神经鞘瘤是罕见的良性肿块,通常发生在颈部区域,但可沿迷走神经的任何部位出现。患者可能无症状,但在大多数情况下,他们在30至60岁出现症状;因此,对于有不明原因心动过缓、吞咽困难、言语不清病史和颈部肿块的患者,应考虑到这种疾病。