Lewis Diedron, Jiménez Laura, Chan Kelvin K, Horton Susan, Wong William W L
School of Pharmacy, University of Waterloo, Waterloo, ON N2G 1C5, Canada.
Department of Community Health and Epidemiology, Dalhousie University, Halifax, NS B3H 4R2, Canada.
Curr Oncol. 2025 Apr 11;32(4):225. doi: 10.3390/curroncol32040225.
Pancreatic cancer (PC) is among the deadliest types of cancer globally. While early detection helps avert adverse outcomes, screening is only recommended for individuals at high risk, specifically those with familial and/or genetic predispositions. The objectives of this study are to systematically review primary studies on the cost-effectiveness of PC screening and to identify the critical factors that influence cost-effectiveness.
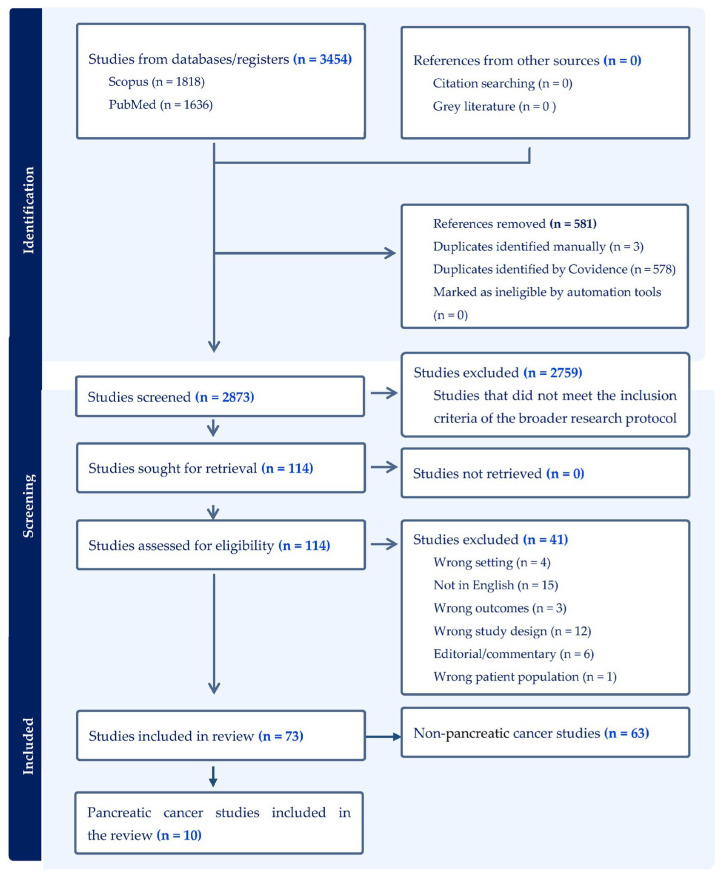
This systematic review was performed using PRISMA guidelines. Economic evaluation studies on PC screening were identified from searches on the SCOPUS and PubMed databases. The quality of reporting of the selected articles was assessed according to CHEERS 2022. Using predefined inclusion and exclusion criteria, two reviewers conducted the title-abstract review, full-text review, and data extraction to select relevant articles. The authors' consensus was used to settle disagreements. The primary outcome was the incremental cost-effectiveness ratio, measured by cost per quality-adjusted life year and cost per life year saved.
Nine studies were selected for the final review. Most studies demonstrated that one-time screening for PC among high-risk individuals was cost-effective compared with no screening, while others found annual screening to also be cost-effective. High-risk was generally defined as having a >5% lifetime risk of PC and included individuals with either familial pancreatic cancer (FPC) or genetic susceptibility syndromes such as Peutz-Jeghers Syndrome, hereditary pancreatitis, hereditary non-polypoid colorectal cancer syndrome, familial adenomatous polyposis, and BRCA2 mutations. Individuals with new-onset diabetes (NOD) were also considered high-risk. Screening using mainly endoscopic ultrasound was cost-effective among FPC individuals and those with genetic syndromes. Risk-based screening was also cost-effective among patients with NOD.
Screening for PC is cost-effective among selected high-risk individuals. However, cost-effectiveness depends on epidemiological factors, cost, the diagnostic performance of screening tools, and the overall design of studies.
胰腺癌(PC)是全球最致命的癌症类型之一。虽然早期检测有助于避免不良后果,但筛查仅推荐给高危个体,特别是那些有家族和/或遗传易感性的个体。本研究的目的是系统评价关于胰腺癌筛查成本效益的原始研究,并确定影响成本效益的关键因素。
本系统评价采用PRISMA指南进行。通过检索SCOPUS和PubMed数据库确定了关于胰腺癌筛查的经济评估研究。根据CHEERS 2022对所选文章的报告质量进行评估。使用预先定义的纳入和排除标准,两名评审员进行标题-摘要评审、全文评审和数据提取,以选择相关文章。作者的共识用于解决分歧。主要结果是增量成本效益比,以每质量调整生命年的成本和每挽救生命年的成本来衡量。
九项研究被选入最终评审。大多数研究表明,与不进行筛查相比,对高危个体进行一次性胰腺癌筛查具有成本效益,而其他研究发现每年筛查也具有成本效益。高危通常定义为胰腺癌终生风险>5%,包括患有家族性胰腺癌(FPC)或遗传易感性综合征(如黑斑息肉综合征、遗传性胰腺炎、遗传性非息肉病性结直肠癌综合征、家族性腺瘤性息肉病和BRCA2突变)的个体。新发糖尿病(NOD)患者也被视为高危个体。主要使用内镜超声进行筛查在FPC个体和患有遗传综合征的个体中具有成本效益。基于风险的筛查在NOD患者中也具有成本效益。
对选定的高危个体进行胰腺癌筛查具有成本效益。然而,成本效益取决于流行病学因素、成本、筛查工具的诊断性能以及研究的总体设计。