Pouplin Alexia, Pham Kormann Diane, Dolivet Gilles, Phulpin Bérengère
Université de Lorraine, CHRU-Nancy, Service d'Odontologie, Département de chirurgie orale, F-54000 Nancy, France; Université de Lorraine, Faculté d'Odontologie, F-54500 Nancy, France.
Institut de Cancérologie de Lorraine, Unité de chirurgie cervico-faciale et dentaire, F-54519 Vandoeuvre-lès-Nancy, France.
Int J Surg Case Rep. 2025 Jun;131:111375. doi: 10.1016/j.ijscr.2025.111375. Epub 2025 Apr 25.
Hemorrhagic shock requiring red blood cell transfusion following tooth extraction is rare.
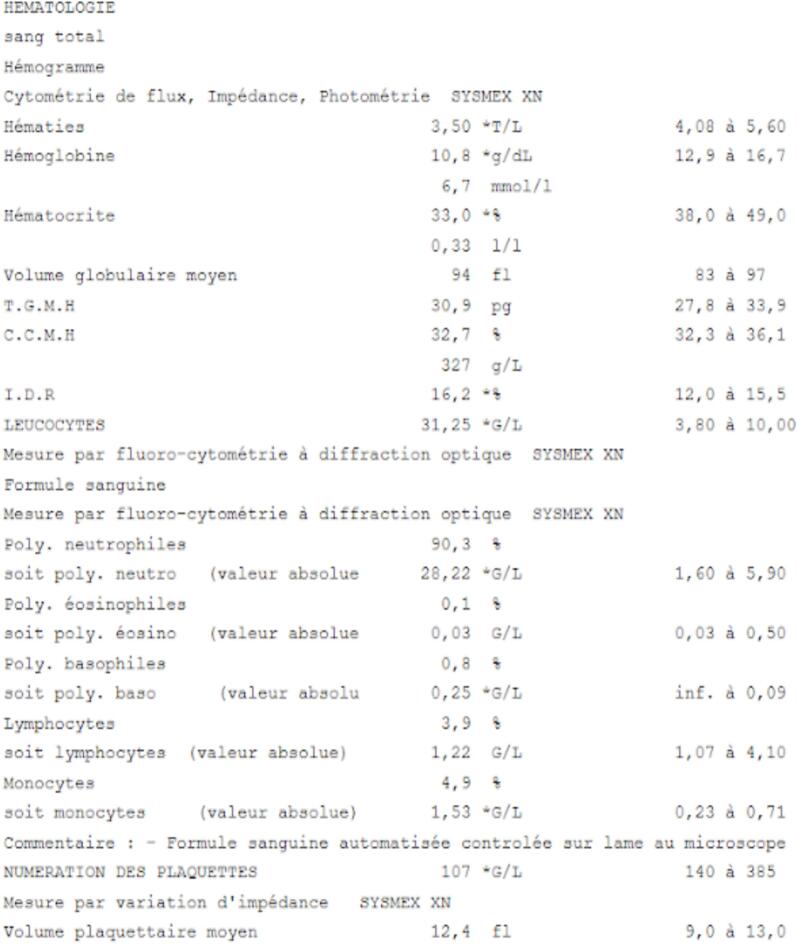
We report the case of a 71-year-old patient who was treated at the hospital for hemorrhagic shock the day after the extraction of two teeth and for a second episode seven days after the surgery. The patient was treated in oncology and his medication included acetylsalicylate of DL-Lysine and Tinzaparine. The pre-operative biological assessment that allowed the surgery and validation of the action to be taken was provided by the cardiologist. Treatment consisted in transfusion and wound revision with controlled hemostasis.
Alveolar bleeding leading to two episodes of hemorrhagic shock (on day 1 and day 7) is an exceptionally rare occurrence. Even if the patient had some risk factors increasing the risks of bleeding, including age, anticoagulants, oncological treatments and recent teeth extractions, no case in the scientific literature was found with similar conditions and no explanation justifying the intensity of the hemorrhage.
Precautions for hemostasis during the intervention are important but sometimes insufficient. For patients at high risk of bleeding with comorbidity like anticoagulant and antiplatelet therapy, it is necessary to establish 7-day postoperative monitoring to control possible post-operative bleeding.
拔牙后需要输注红细胞的出血性休克很少见。
我们报告一例71岁患者的病例,该患者在拔除两颗牙齿后的第二天因出血性休克在医院接受治疗,并在手术后七天出现第二次出血性休克发作。该患者接受肿瘤治疗,其用药包括赖氨匹林和亭扎肝素。手术前的生物学评估由心脏病专家提供,该评估允许进行手术并确认所采取的措施。治疗包括输血和伤口修复并控制止血。
导致两次出血性休克发作(第1天和第7天)的牙槽出血极为罕见。即使患者有一些增加出血风险的危险因素,包括年龄、抗凝剂、肿瘤治疗和近期拔牙,但在科学文献中未发现有类似情况的病例,也没有能解释出血强度的原因。
干预期间的止血预防措施很重要,但有时并不充分。对于有抗凝和抗血小板治疗等合并症的高出血风险患者,有必要进行术后7天的监测以控制可能的术后出血。