Andeen Nicole K, Kung Vanderlene L, Nguyen Jane K, Avasare Rupali S, Nakhoul Georges N, Shrestha Nabin K, Makadia Jina T, Jesperson Tricia, Nast Cynthia C, Choung Grace Hae Yoon, Herlitz Leal
Department of Pathology and Laboratory Medicine, Oregon Health and Science University, Portland, Oregon, USA.
Department of Pathology, Cleveland Clinic, Cleveland, Ohio, USA.
Kidney Int Rep. 2025 Jan 16;10(4):1237-1247. doi: 10.1016/j.ekir.2025.01.009. eCollection 2025 Apr.
are highly fastidious gram-negative facultative intracellular bacteria which can cause a culture-negative infective endocarditis (IE) with unique clinicopathologic features.
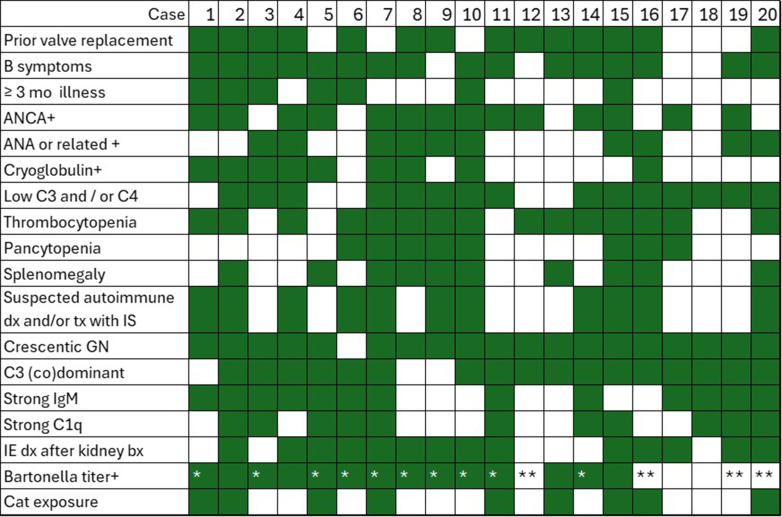
In this study, we assembled 20 cases of glomerulonephritis (GN) due to IE from 3 institutions and compared them with 49 cases of culture-positive IEGN and 30 cases of non-endocarditis infection-related GN (IRGN).
IEGN was seen in approximately 0.15% to 0.4% of native renal biopsies, with causing 8% to 21% of IEGN. Patients with IEGN had preexisting cardiac valve alterations (75%); antineutrophil cytoplasmic autoantibody (ANCA) positivity (67%); hypocomplementemia (75%); antinuclear antibody positivity (53%); cryoglobulinemia (45%); and hematologic manifestations, including B-symptoms (79%), splenomegaly (59%), thrombocytopenia (83%), and pancytopenia (44%). In 75% of the cases, endocarditis was not diagnosed until after kidney biopsy. Pathologically, IEGN presented as a focally crescentic GN, which was C3 codominant (80%) with strong IgM (65%) and/or C1q (55%), or pauci-immune (10%), with predominantly mesangial deposits and limited exudative features. At a median follow-up time of 15 months, progression to end-stage kidney disease (ESKD) for all-comers with IEGN was associated with higher creatinine levels at diagnosis, presence of nephrotic syndrome, female sex, and C1q staining intensity. Although delayed diagnosis of infection and immunosuppressive therapy for presumed autoimmune disease before kidney biopsy were more common in IEGN than in culture-positive IEGN, neither were associated with ESKD.
IEGNs share laboratory and biopsy features with autoimmunity, which may obfuscate identification of underlying bacterial infection.
是高度苛求的革兰氏阴性兼性细胞内细菌,可导致具有独特临床病理特征的培养阴性感染性心内膜炎(IE)。
在本研究中,我们收集了来自3家机构的20例因IE导致的肾小球肾炎(GN)病例,并将其与49例培养阳性的IEGN病例和30例非心内膜炎感染相关GN(IRGN)病例进行比较。
IEGN在约0.15%至0.4%的原发性肾活检中可见,导致8%至21%的IEGN。IEGN患者有既往心脏瓣膜改变(75%);抗中性粒细胞胞浆自身抗体(ANCA)阳性(67%);低补体血症(75%);抗核抗体阳性(53%);冷球蛋白血症(45%);以及血液学表现,包括B症状(79%)、脾肿大(59%)、血小板减少(83%)和全血细胞减少(44%)。在75%的病例中,直到肾活检后才诊断出心内膜炎。病理上,IEGN表现为局灶性新月体性GN,C3共显性(80%),伴有强IgM(65%)和/或C1q(55%),或寡免疫性(10%),主要为系膜沉积且渗出特征有限。在中位随访时间15个月时,所有IEGN患者进展至终末期肾病(ESKD)与诊断时更高的肌酐水平、肾病综合征的存在、女性性别和C1q染色强度相关。尽管在肾活检前对感染的延迟诊断和对假定自身免疫性疾病的免疫抑制治疗在IEGN中比在培养阳性的IEGN中更常见,但两者均与ESKD无关。
IEGN与自身免疫有共同的实验室和活检特征,这可能会混淆潜在细菌感染的识别。