Lee Junwoo, Choi Jaehwan, Kang Min Seok, Yu Seung-Young, Kim Kiyoung
Department of Ophthalmology, Gachon University Gil Medical Center, Incheon, Korea.
Department of Ophthalmology, Kyung Hee University Hospital, Kyung Hee University, 23, Kyungheedae-ro, Dongdaemun-gu, Seoul, 02447, Republic of Korea.
BMC Ophthalmol. 2025 Apr 30;25(1):262. doi: 10.1186/s12886-025-04102-y.
A combination of FOLFOX and nivolumab is a first-line treatment for HER2-negative advanced gastric cancer, significantly improving survival. However, this regimen is associated with potential neurotoxicity. 5-Fluorouracil and oxaliplatin in FOLFOX have been linked to optic neuropathy, whereas nivolumab, an immune checkpoint inhibitor, may cause immune-related optic neuropathy. Although FOLFOX plus nivolumab provides considerable survival benefits, careful monitoring for ocular complications is essential. We report a case of bilateral optic neuropathy in a patient who received FOLFOX plus nivolumab. Despite discontinuation of chemotherapy and treated with high-dose corticosteroid pulse therapy, the patient's symptoms did not improve.
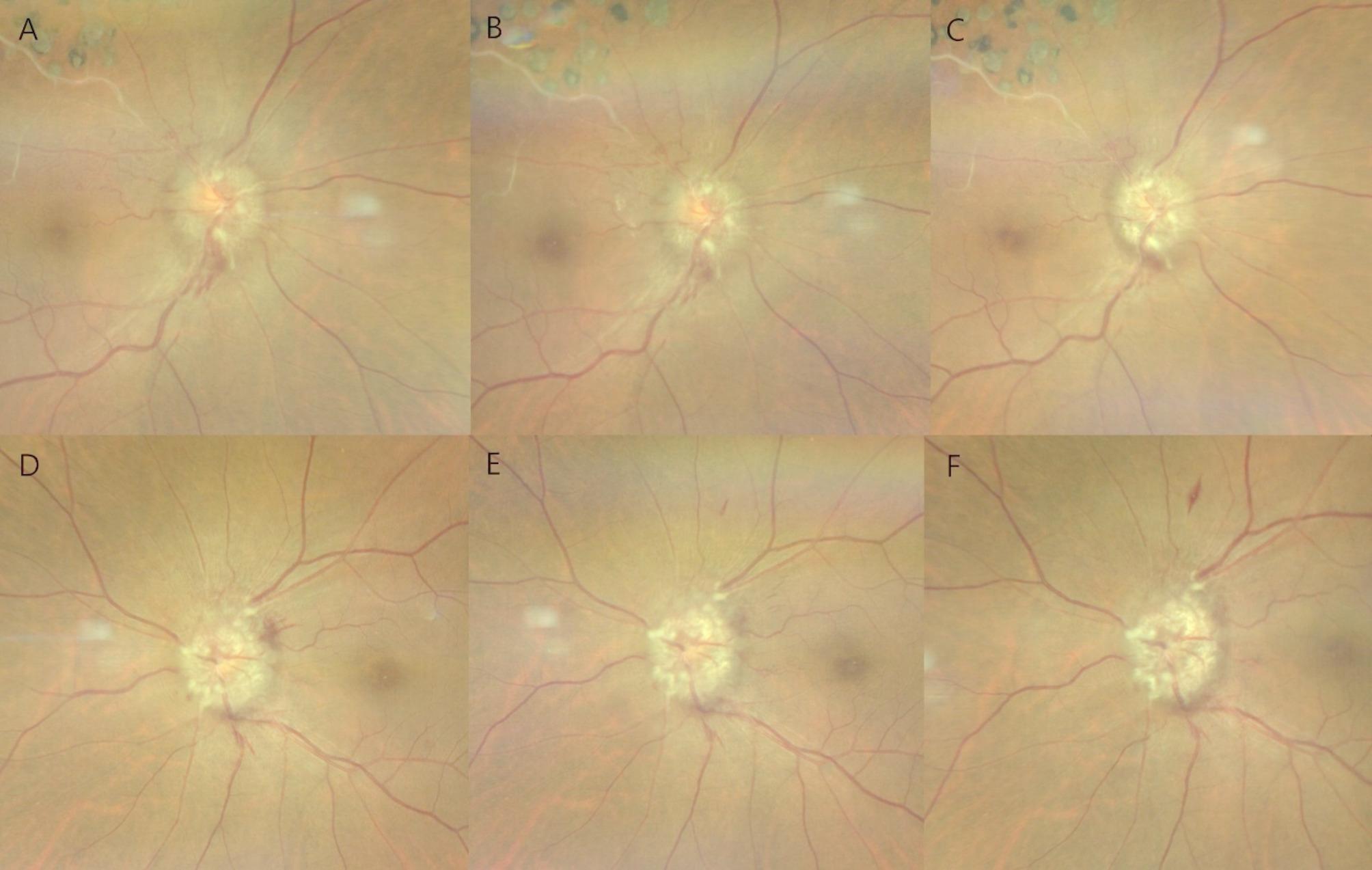
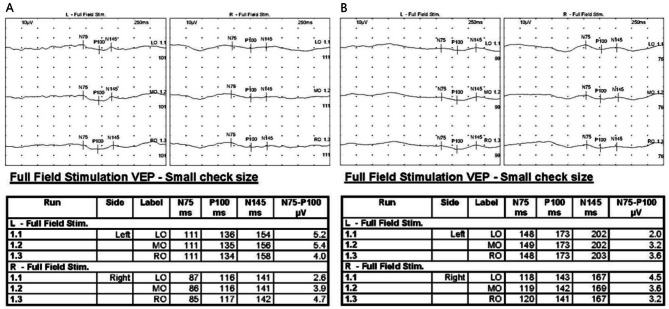
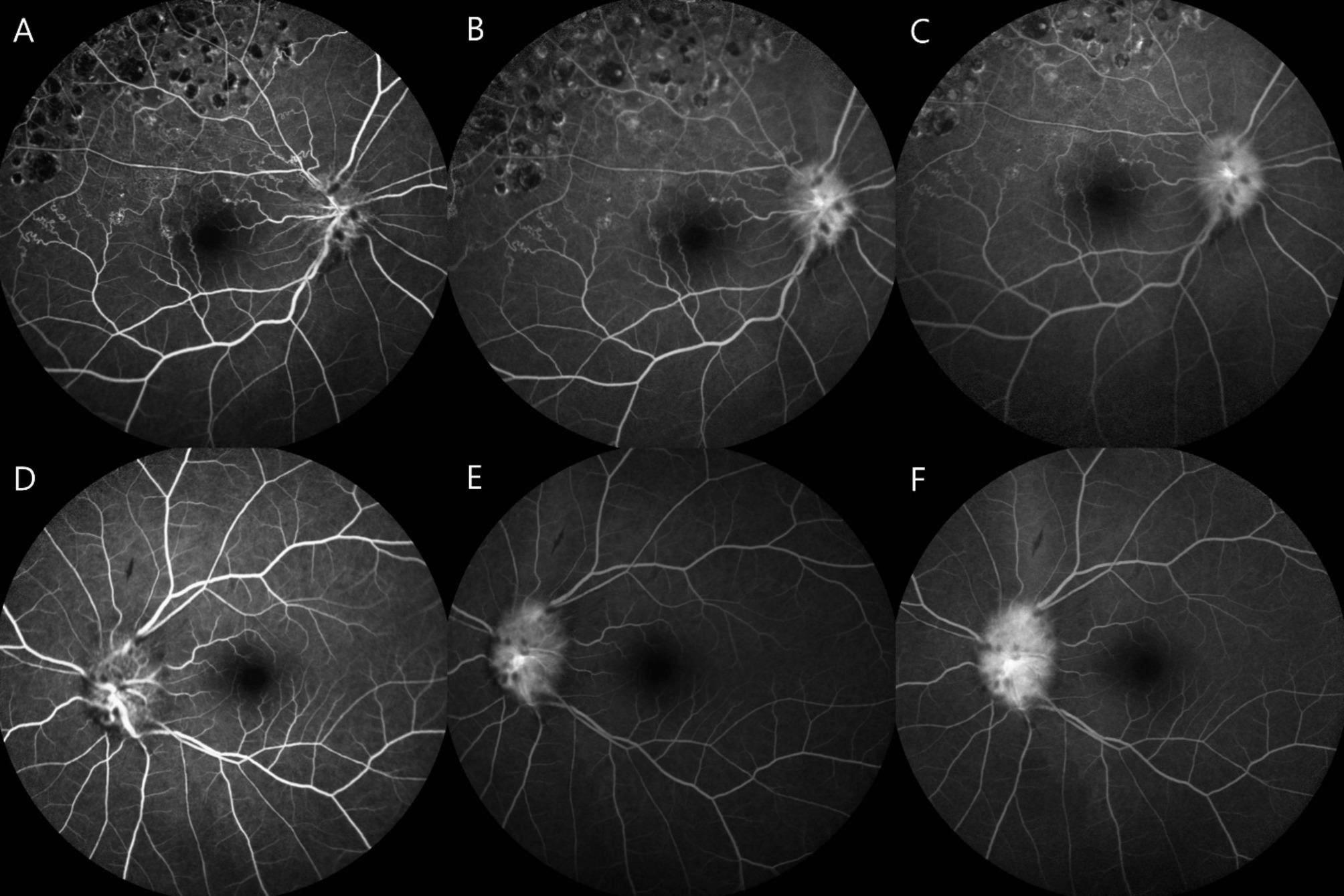
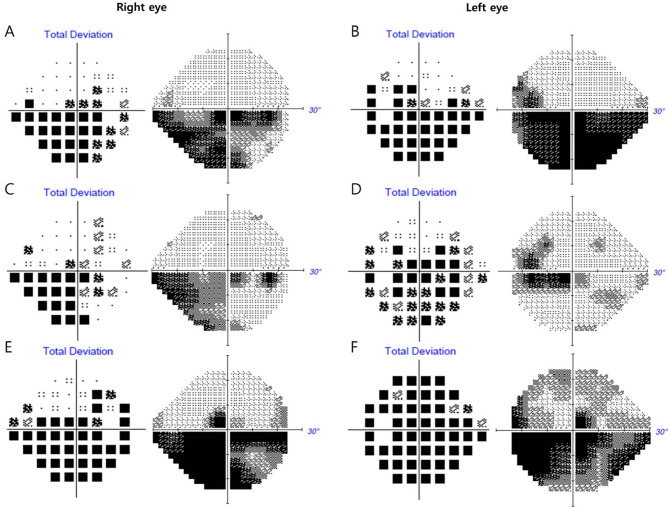
A 48-year-old woman with a Krukenberg tumor developed progressive bilateral visual impairment during treatment with FOLFOX plus nivolumab. Her ophthalmologic history included branch retinal vein occlusion in the right eye but no systemic diseases. She presented with bilateral central scotomas and visual field defects. On examination, best-corrected visual acuity (BCVA) was 20/40 in the right eye and 20/25 in the left eye, with bilateral optic disc swelling and hemorrhage. Fluorescein angiography confirmed optic disc leakage, and a visual evoked potential (VEP) test indicated axonal loss. Brain magnetic resonance imaging (MRI) and positron emission tomography-computed tomography (PET-CT) ruled out metastatic disease, and autoimmune markers were negative. High-dose intravenous methylprednisolone was administered, and chemotherapy was discontinued. Despite initial stabilization, vision deteriorated, ultimately progressing to light perception in both eyes. Repeated steroid pulse therapy failed to improve outcomes.
This case highlights the potential for severe bilateral optic neuropathy associated with FOLFOX plus nivolumab, leading to irreversible vision loss. These findings suggest that close ophthalmologic monitoring is warranted in patients receiving FOLFOX plus nivolumab for early recognition of bilateral visual impairment. Further research is needed to elucidate the mechanisms and identify agents responsible for the development of optic neuropathy.
FOLFOX方案与纳武单抗联合使用是HER2阴性晚期胃癌的一线治疗方案,可显著提高生存率。然而,该方案存在潜在的神经毒性。FOLFOX方案中的5-氟尿嘧啶和奥沙利铂与视神经病变有关,而免疫检查点抑制剂纳武单抗可能导致免疫相关性视神经病变。尽管FOLFOX联合纳武单抗可带来显著的生存获益,但仔细监测眼部并发症至关重要。我们报告一例接受FOLFOX联合纳武单抗治疗的患者发生双侧视神经病变的病例。尽管停用了化疗并接受了大剂量糖皮质激素冲击治疗,但患者症状并未改善。
一名患有库肯勃瘤的48岁女性在接受FOLFOX联合纳武单抗治疗期间出现进行性双侧视力损害。她的眼科病史包括右眼分支视网膜静脉阻塞,但无全身性疾病。她表现为双侧中心暗点和视野缺损。检查时,右眼最佳矫正视力(BCVA)为20/40,左眼为20/25,双侧视盘肿胀和出血。荧光素血管造影证实视盘渗漏,视觉诱发电位(VEP)测试表明存在轴突损失。脑部磁共振成像(MRI)和正电子发射断层扫描-计算机断层扫描(PET-CT)排除了转移性疾病,自身免疫标志物为阴性。给予大剂量静脉注射甲泼尼龙,并停用化疗。尽管最初病情稳定,但视力仍恶化,最终发展为双眼仅存光感。重复的激素冲击治疗未能改善预后。
本病例突出了FOLFOX联合纳武单抗相关的严重双侧视神经病变的可能性,可导致不可逆的视力丧失。这些发现表明,对于接受FOLFOX联合纳武单抗治疗的患者,有必要进行密切的眼科监测,以便早期识别双侧视力损害。需要进一步研究以阐明其机制并确定导致视神经病变的因素。