de Matos Leonor Vasconcelos, Louro Tatiana, Padrao Teresa Gantes, Debiasi Marcio, Sousa Berta, Gouveia Helena, Cardoso Fatima
Breast Unit, Champalimaud Clinical Center, Champalimaud Foundation, Avenida de Brasília, S/N, 1400-038, Lisbon, Portugal.
Support Care Cancer. 2025 May 5;33(6):449. doi: 10.1007/s00520-025-09502-w.
Timely and integrated palliative care is crucial for patients with metastatic breast cancer. However, data on models of integration are scarce. We aimed to evaluate the impact of the integration of an embedded model of palliative care in a multidisciplinary breast unit on important goals of care and to characterize different patterns of integration (palliative predominant, oncology predominant or concurrent).
Single-center, retrospective, observational cohort study including all patients with metastatic breast cancer followed by the palliative and oncology teams from a 12-month period before (pre-implementation) and after (post-implementation) of an embedded model of integration of palliative care. We analyzed early integration, 1-year survival rate, survival and different patterns of coordination of palliative care and oncology (the oncology-predominant pattern, the palliative care-predominant pattern and the concurrent integrated care pattern).
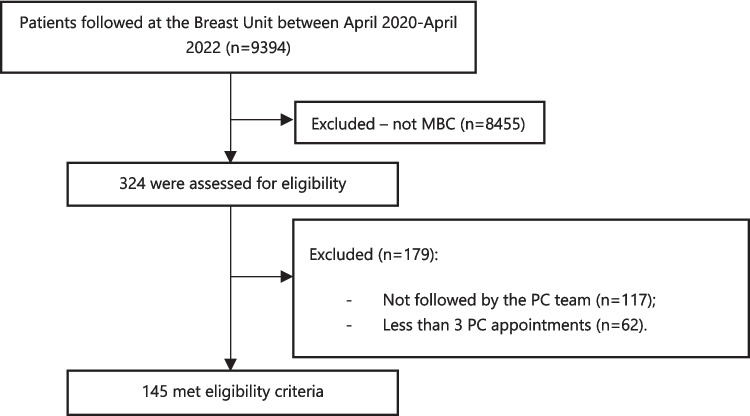
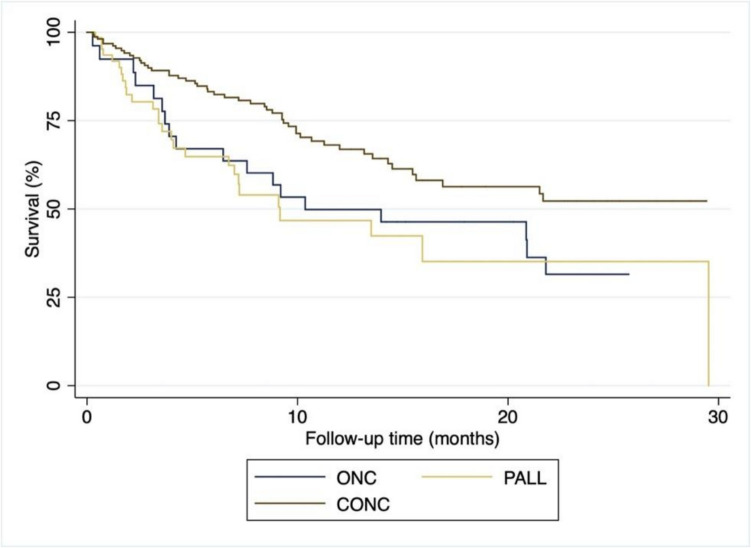
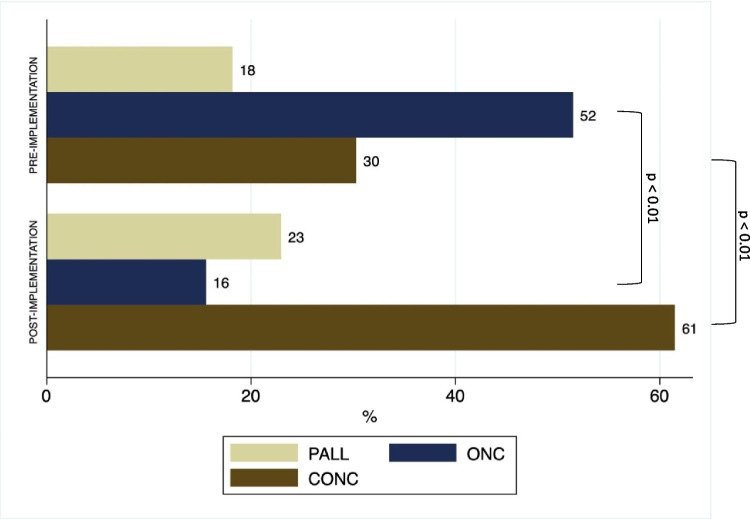
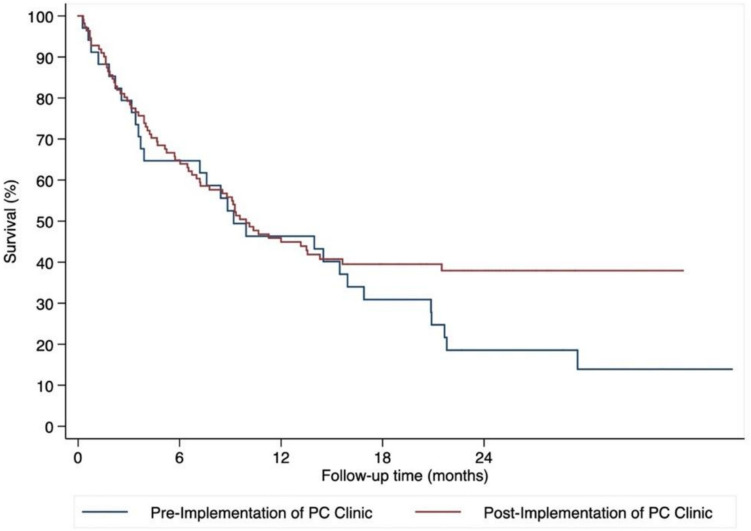
From April 2020 to April 2022, a total of 145 patients were included in the analysis: all female, median age of 63.5 years, 20.7% with triple negative disease. Post-implementation, early referrals significantly increased (35.3 to 61.3%, p < 0.01), 1-year survival rate (40.1% vs 40.7%) and survival time were similar (9.2 months vs 9.9 months). An integrated pattern of care with concurrent palliative and oncology appointments was significantly more frequent (30% vs 61%, p < 0.01). When compared to the other patterns, the concurrent pattern was associated to a median of 4 months longer survival (p < 0.01).
The incorporation of an embedded model of palliative care was associated with earlier referrals and translated into better outcomes for patients with metastatic breast cancer.
及时且综合的姑息治疗对转移性乳腺癌患者至关重要。然而,关于整合模式的数据却很匮乏。我们旨在评估在多学科乳腺科中嵌入姑息治疗模式对重要护理目标的影响,并描述不同的整合模式(姑息治疗为主、肿瘤学为主或并行)。
单中心、回顾性、观察性队列研究,纳入了在姑息治疗与肿瘤学团队随访下的所有转移性乳腺癌患者,研究时间为嵌入姑息治疗整合模式实施前(实施前)和实施后(实施后)的12个月期间。我们分析了早期整合情况、1年生存率、生存期以及姑息治疗与肿瘤学的不同协调模式(肿瘤学为主模式、姑息治疗为主模式和并行综合护理模式)。
2020年4月至2022年4月,共有145例患者纳入分析:均为女性,中位年龄63.5岁,20.7%为三阴性疾病。实施后,早期转诊显著增加(从35.3%增至61.3%,p<0.01),1年生存率(40.1%对40.7%)和生存时间相似(9.2个月对9.9个月)。姑息治疗与肿瘤学预约并行的综合护理模式显著更频繁(30%对61%,p<0.01)。与其他模式相比,并行模式的生存期中位数长4个月(p<0.01)。
纳入嵌入的姑息治疗模式与更早转诊相关,并为转移性乳腺癌患者带来了更好的结果。